1.Introduction
Telehealth has emerged as a transformative force in healthcare, with the potential to improve the quality of healthcare and save lives.[1,2] Telehealth is typically characterized as the use of telecommunications and information technology (IT) to provide remote access to a health assessment, diagnosis, intervention, consultation, supervision, and information.[2] While there is limited research on the effects of telehealth interventions on timely patient discharge, length of stay (LOS), and discharge timing, many healthcare organizations have implemented telehealth strategies to monitor patients post-discharge,[1,3] prevent hospitalization, reduce readmission,[4—6] and ensure patients comply with prescription regimens.[7,8] Evidence from these studies suggests that telehealth can significantly enhance care transitions after hospital discharge, patient involvement, and medication adherence.
Given the potential of telehealth to enhance care transitions, it may also play a role in addressing factors that hinder timely hospital discharges. Many healthcare institutions face challenges in discharging patients promptly due to issues such as communication breakdowns, undefined processes, delays in receiving test results, slow execution of discharge orders, and issues related to determining discharge destinations.[9—12] These barriers contribute to discharge delays across various settings. Delays in discharging patients could contribute to an extended LOS, leading to dissatisfied patients and family members, as well as an increased risk of contracting hospital-acquired infections and congesting patient throughput.[13,14] As a means of contributing to increased satisfaction, healthcare organizations are continually striving to improve patient discharge efficiency and reduce LOS by implementing various strategies such as using multidisciplinary teams, interdisciplinary rounding processes, and a lean and six-sigma approach.[10,11,15,16] However, as various organizations are moving towards enhanced discharge planning and reducing LOS, one such intervention that should be considered is the use of telehealth through virtual nursing, with nurses remotely monitoring patients and providing support to nurses physically caring for patients in the unit. Telehealth, particularly reinforced during the COVID-19 pandemic, has shown potential for enhancing patient and family satisfaction by providing cost-effective, high-quality care.[17,18]
We deployed virtual nursing in a tele-acute unit of an academic medical center (AMC) located in the southeastern United States. Virtual nurses were required to have a minimum of two years of clinical experience, and, in addition to patient interventions, were charged with mentoring any newly graduated nurses performing bedside care for patients on the telehealth unit. The interventions of the virtual nurses were aimed at increasing efficiency and timeliness, while decreasing the workload of the bedside nurse. The virtual nurse involvement included assisting with completing most of the intake process and risk assessments including pressure ulcers, falls, deep vein thrombosis, and peptic ulcer disease, in addition to completing virtual rounds to assess patient needs and environment. These interventions reduced pressure injuries by 60% and falls by 65% in the tele-acute unit, according to internal quality improvement studies. Virtual nurses assisted with lab review through communicating critical and concerning labs to the bedside team and monitoring blood glucose levels and treatments. Additionally, the virtual nurses helped with assessments that included level of comfort, pain assessment, and restraints. The telehealth nurses were also involved in ensuring the accuracy of medication orders and delivery by assessing if the physician orders matched the notes concerning the patient’s plan of care and what the patient is receiving, as well as checking for duplicate orders, medication compliance, and any contraindications between medications and patient condition. Finally, the telehealth nurses assisted with medication reconciliation as part of the admission process, in addition to providing any necessary medication education to patients and families throughout their inpatient stay. Given that discharge planning should begin at admission, we predicted that these telehealth interventions would positively impact the timeliness of the discharge process by allowing the bedside nurse to better focus on discharge promoters and barriers.
In this study, we aim to examine the impact of virtual nursing interventions on LOS and ratio of LOS to risk-adjusted-LOS (RAE-LOS) in a tele-acute unit and a traditional unit. We hypothesize that a tele-acute intervention in nursing care led to better clinical outcomes, specifically in terms of LOS and the ratio of actual LOS to RAE-LOS. For LOS, we examine the difference between actual LOS and RAE-LOS, with RAE-LOS being projected by a Vizient® risk-adjusted model based on individual patient billing codes and demographic information.
2.Methods
2.1Data collection
Retrospective data were collected from a tele-acute and traditional units from an AMC located in the southeastern United States. A total of 6,999 visits were obtained between the second quarter of 2020 and the fourth quarter of 2023. The distribution of visits between the tele-acute unit and traditional unit is 3,679 and 3,320, respectively. Each encounter in the data represents a patient visit, with duplicate visits counting as unique encounters, and includes admission and discharge dates, actual LOS, RAE-LOS, time from order to discharge, and the type of inpatient unit. The ratio between actual LOS and RAE-LOS is calculated. If the ratio is larger than 1, it means a patient stayed more time than projected, and if it is less than 1, it means the patient stayed less time than projected. Prior to performing the tests and regression analysis, missing values and outliers were identified and removed, resulting in a dataset of 135 observations. Summary statistics of the cleaned data are included in Table 1.
| Order to discharge min | 847.10 ± 3,319.30 (2.73-27,506.03) |
|
| LOS | 7.26 ± 4.10 (0.92-18.81) |
|
| Risk adj LOS | 6.48 ± 2.43 (2.17-12.59) |
|
| Ratio | 1.18 ± 0.68 (0.25-5.01) |
|
| Nurse Unit | Tele-Acute | 63.18% |
| Traditional | 36.82% | |
| Readmission Risk Score | High Risk | 41.36% |
| Low Risk | 23.18% | |
| Moderate Risk | 18.64% | |
| Not Appropriate | 16.82% | |
| Living Situation | With Family | 72.86% |
| Alone | 22.11% | |
| Other | 5.03% | |
| Insurance Group | Government Programs | 66.82% |
| Commercial Insurances | 26.82% | |
| Financial Assistance | 5.91% | |
| Other | 0.45% | |
2.2Statistical analysis
The statistical analysis was conducted in two steps. First, a bivariate analysis was performed by comparing the mean LOS and the ratio of LOS to RAE-LOS for the two units (tele-acute and traditional) using line charts at quarterly bands. Additionally, the Mann-Whitney
In the second step, multivariate linear regression was conducted to analyze the factors affecting both LOS and the ratio. This analysis aimed to quantify the impact of various variables, including hospital setting and readmission risk score, on LOS and the ratio. Log transformation was applied to the dependent variables to achieve normally distributed residuals.
2.3Mann-Whitney
The goal of the analysis was to determine whether there was a significant difference between the two units (tele-acute and traditional) with respect to the actual LOS and the ratio of LOS to RAE-LOS. Since the data were collected from the same hospital, it is assumed that the two units have equal variance. The Shapiro-Wilk test confirmed that LOS and the ratio are not normally distributed. Therefore, the Mann-Whitney
- Null Hypothesis (H0): The LOS and ratio for tele-acute unit are not significantly less than for the traditional unit.
- Alternative Hypothesis (H1): The LOS and ratio for tele-acute unit are significantly less than for traditional unit.
2.4Multivariate regression
To further investigate the relationship between the dependent variables (LOS and ratio) and independent variables (hospital setting), two multivariate linear regression analyses were conducted at the encounter level. The regression models aim to quantify the effect of each variable on LOS and ratio. The regression analysis helps to understand how the hospital setting influences the dependent variables (LOS, ratio) and to quantify the magnitude of these effects.
3.Results
3.1Line chart comparison
Line charts were used to compare the LOS and the ratio of LOS to RAE-LOS between the tele-acute and traditional units banded by quarter. Figure 1 shows the quarterly changes in the ratio of LOS to RAE-LOS for both units from Q2 2022 to Q4 2023. Overall, the ratio for the tele-acute unit is lower than the traditional unit across most quarters, indicating that the tele-acute patients stay less time than predicted. This is also explained by the actual LOS chart in Figure 2 for both units over the same period. Figure 2 shows that the LOS for tele-acute patients remains lower than that for traditional patients in most quarters, suggesting that patients in the tele-acute unit tend to have shorter stays compared to those in the traditional unit.
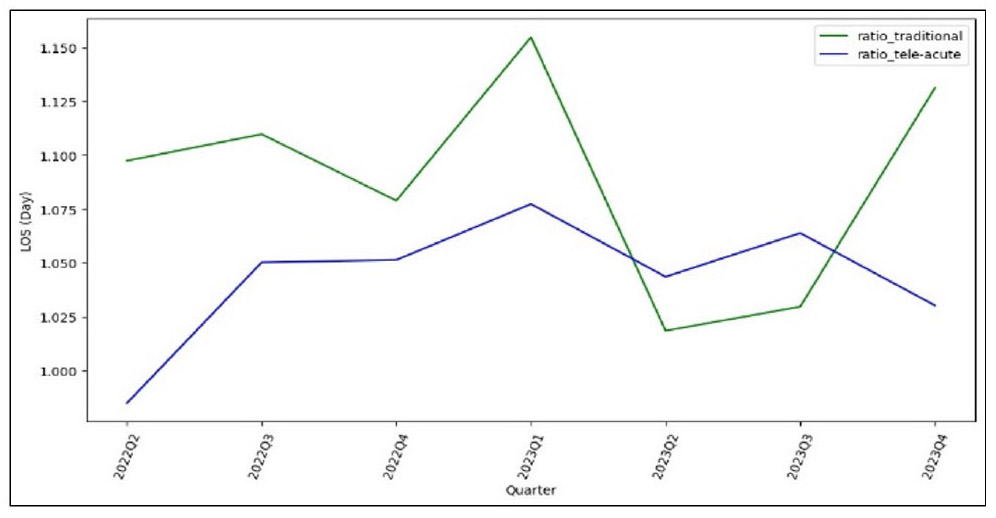
Figure 1.
Mean of Ratio of tele-acute vs. traditional per quarter
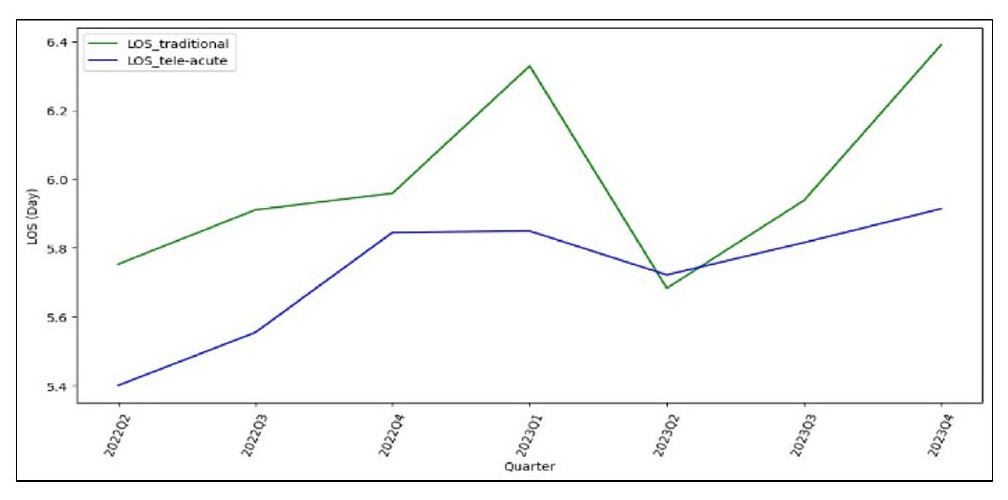
Figure 2.
Mean LOS of tele-acute vs. traditional per quarter
3.2Mann-Whitney
The Mann-Whitney
| Length of Stay (LOS) | 1,640,020 | 0.17 | Not significantly greater (traditional) |
| Ratio (LOS/risk-adjusted LOS) | 1,677,373 | 0.015 | Significantly less (tele-acute) |
3.3Multivariate linear regression results
Two multivariate regression models were developed at the encounter level, focusing on LOS and the ratio of LOS to RAE-LOS, respectively. Log transformation was applied to the dependent variables to achieve normally distributed residuals.
3.4LOS model
For the LOS model, the “Nurse Unit” variable had a statistically significant positive coefficient (Coefficient = 0.319,
| Nurse Unit | 0.319 | .001 |
|
0.214 | .007 |
|
|
| Order to Discharge (min) | 0.000 | .436 | ns | 0.000 | .718 | ns | |
| Readmission Risk Score (base = High Risk) | Low Risk | 0.028 | .806 | ns | 0.075 | .441 | ns |
| Moderate Risk | -0.098 | .414 | ns | -0.070 | .491 | ns | |
| Not Appropriate | 0.288 | .183 | ns | 0.187 | .310 | ns | |
| Living Situation (base = Alone) | Other | 0.108 | .627 | ns | -0.085 | .655 | ns |
| With Family | 0.067 | .488 | ns | -0.020 | .806 | ns | |
| Insurance Group (base = Commercial Insurances) | Financial Assistance | 0.157 | .426 | ns | 0.055 | .745 | ns |
| Government Programs | -0.089 | .351 | ns | -0.168 | .040 |
|
|
| Other | -0.069 | .881 | ns | 0.069 | .860 | ns | |
| 0.896 | 0.10 | ||||||
The “Order to Discharge” variable did not show statistical significance related to the log-transformed LOS (Coefficient = 0.000,
Living situation and insurance group generally did not have statistically significant effects on the log-transformed LOS. The exceptions were that “financial assistance” and “government programs” had no statistically significant impact on LOS compared to commercial insurance, while being in the “Other” insurance category also did not significantly affect the log-transformed LOS.
3.5Risk-adjusted ratio model
For the risk-adjusted ratio model, the “Nurse Unit” variable had a statistically significant positive coefficient (Coefficient = 0.214,
The “Order to Discharge” variable did not have a statistically significant affect on the log-transformed ratio (Coefficient = 0.000,
Living situation did not demonstrate statistical significance related to the log-transformed ratio. Categories “Other” and “With Family” had coefficients of -0.085 (
The
4.Discussion
This study examined the impact of virtual nursing in a tele-acute care unit in a large AMC in the southeastern United States relative specifically to time from order to discharge, LOS, and the ratio of actual LOS and RAE-LOS. To do this, we compared two acute care units: tele-acute and traditional. This study contributes to a body of literature that is lacking in the use of telehealth nursing in the acute care setting, and more specifically its contribution in transitions of care. Our findings are indirectly consistent with the literature demonstrating various improvements across the care continuum post-discharge.[1,3,7,8] Our research offers new perspectives on how telehealth can affect operational measures like LOS and discharge times. This contribution is important as it broadens the scope of telehealth’s benefits beyond traditional remote care, highlighting its potential in fast-paced, acute care settings.
Our findings indicate that telehealth interventions in the tele-acute unit demonstrate statistically significantly impact the LOS and the ratio of actual LOS to RAE-LOS compared to the traditional unit. We observed in consecutive quarters that patients stayed shorter than projected in the tele-acute unit compared to the traditional unit. We conducted two different analyses using the LOS Model and the Ratio Model. These models were applied at the encounter level to examine the relationship between LOS and the ratio of actual to RAE-LOS across both units (tele-acute and traditional).
The findings from the LOS Model showed that the tele-acute unit had a shorter LOS than the traditional unit. There are several indirect implications on healthcare delivery and outcomes. Prolonged hospital stays, as documented in the literature, are associated with an increased risk of hospital-acquired infection and adverse patient outcomes.[19] Insurers often do not cover the costs associated with these extended stays and consequent complications, thereby financially impacting hospitals.[19] The average daily cost of an acute care bed at the institution is between $1,200 and $1,500, per departmental leadership. Our study showed that the LOS in the traditional unit was 1.38 times longer than in the tele-acute unit. Based on these figures, the potential daily cost implication ranges from approximately $1,656-$2,070 per admission. Furthermore, a longer LOS in the hospital exacerbates throughput challenges, leading to a bottleneck effect.[12,16] This bottleneck effect causes patients in the emergency department to face delays in admission or even initial evaluations due to the unavailability of beds downstream on the care units.[12,16]
There is also an indirect impact on emergency department operations and staff well-being. If patients stay longer in these units, ER nurses will be required to manage acute care patients for extended periods, which diverges from their primary training in rapid patient assessment and stabilization. This misalignment in job function may lead to increased stress and burnout, negatively affecting staff retention rates.[20] This underscores the importance of strategically improving patient flow and resource allocation to enhance overall healthcare efficiency and quality.
On the Ratio Model, we also found that being in the tele-acute unit was associated with a lower log-transformed ratio of LOS to RAE-LOS compared to the traditional unit. The model also showed that patients stayed shorter than expected in the tele-acute unit compared to the traditional unit. This finding suggests that discharge planning should be initiated at the time of admission to reduce potential unexpected extended stays, which is consistent with the literature.[12,16,21,22] Additionally, increasing resources, such as employing more tele-nurses, might improve efficiency and patient flow in the traditional units. However, the ratio model should be interpreted cautiously, as only 10% of the variance in the ratio is explained by the variables included in the model.
In light of the findings, this study had some limitations. This study was conducted in an AMC. AMCs are often thought to be resource rich with study findings that are not generalizable beyond the AMC environment. The impact of tele-interventions on LOS might be more pronounced in a lower resource setting. The study was conducted in the southeastern United States, potentially limiting generalizability to other geographic regions. The representativeness of our findings may be limited due to a substantial reduction in our data sample caused by numerous missing variables. This reduction in sample size could affect our results’ reliability and generalizability, as well as the findings themselves. Additionally, the ratio model had an
5.Conclusion
This study makes a strong association between the use of telehealth nurses and LOS and the ratio of LOS to RAE-LOS. These findings show that integrating telehealth may contribute to more efficient patient management, leading to earlier discharges and potentially reducing the burden on healthcare systems. Our findings add valuable insights to the emerging literature on telehealth applications in acute care, demonstrating that telehealth can significantly improve operational efficiencies such as discharge times and LOS. Overall, this study underscores the significant potential of telehealth to transform acute care delivery, improve patient outcomes, and optimize hospital resource utilization.
Authors contributions
SSF, EW, TS, AA and EEB originally conceptualized the project. AA analyzed data and wrote applicable parts of the paper. EEB and GO wrote the initial paper draft and managed edits and revisions of drafts. JB was responsible for data extraction. EW, WS, TS, and BK served as content experts. SSF was responsible for study oversight. All authors reviewed and approved all manuscript drafts.
Funding
The research is supported by the University of Alabama at Birmingham eMedicine Research Collaborative.
Conflicts of Interest Disclosure
The authors declare they have no conflicts of interest.
Informed consent
Due to the retrospective nature of the research, informed consent was not collected.
Ethics statement
This study was approved by the Institutional Review Board of The University of Alabama at Birmingham (No. IRB-300008433) and was conducted per the ethical principles of the Declaration of Helsinki.
Ethics approval
The Publication Ethics Committee of the Sciedu Press. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
Data utilized in this study is not publicly available due to privacy or ethical considerations. Data may be available upon request to the corresponding author.
Data sharing statement
No additional data are available.
Acknowledgements
The authors acknowledge the expert revisions suggested by the reviewers. those revisions helped to provide clarity to this study and resulted in an overall better manuscript.
References
- Snoswell C, Taylor M, Comans T. Determining if Telehealth Can Reduce Health System Costs: Scoping Review. J Med Internet Res. 2020;22(10):e17298. doi:10.2196/17298
- Kichloo A, Albosta M, Dettloff K. Telemedicine, the current COVID-19 pandemic and the future: a narrative review and perspectives moving forward in the USA. Fam MedCommunity Health. 2020;8(3):e000530.
- Hoppe K, Williams M, Thomas N. Telehealth with remote blood pressure monitoring for postpartum hypertension: a prospective single-cohort feasibility study. Pregnancy hypertension. 2019;15:1716.
- Langabeer J, Gonzalez M, Alqusairi D. Telehealth-enabled emergency medical services program reduces ambulance transport to urban emergency departments. Western Journal of Emergency Medicine. 2016;17(6):713.
- Gillespie S, Shah M, Wasserman E. Reducing emergency department utilization through engagement in telemedicine by senior living communities. Telemedicine and e-Health. 2016;22(6):489-96. doi:10.1089/tmj.2015.0152
- O’Connor M, Asdornwised U, Dempsey M. Using telehealth to reduce all-cause 30-day hospital readmissions among heart failure patients receiving skilled home health services. Applied Clinical Informatics. 2016;7(02):238-47.
- Wakefield B, Holman J, Ray A. Outcomes of a home telehealth intervention for patients with heart failure. Journal of Telemedicine and Telecare. 2009;15(1):46-50. doi:10.1258/jtt.2008.080701
- Cole J, Wilkins N, Moss M. Impact of pharmacist involvement on Telehealth Transitional Care Management (TCM) for high medication risk patients. Pharmacy. 2019;7(4):158. doi:10.3390/pharmacy7040158
- Wertheimer B, Jacobs R, Bailey M. Discharge before noon: an achievable hospital goal. J Hosp Med. 2014;9(4):210-4.
- Kane M, Weinacker A, Arthofer R. A multidisciplinary initiative to increase inpatient discharges before noon. Journal of Nursing Administration. 2016;46(12):630-5. doi:10.1097/NNA.0000000000000418
- Patel H, Yirdaw E, Yu A. Improving Early Discharge Using a Team-Based Structure for Discharge Multidisciplinary Rounds. Prof Case Manag. 2019;24(2):83-9. doi:10.1097/NCM.0000000000000318
- Feldman S, Kennedy K, Nafziger S. Critical Success Factors for Addressing Discharge Inefficiency at a Large Academic Medical Center: A Lean Six Sigma Approach. Journal of Nursing Care Quality. 2022;37(2):135-41.
- Micallef A, Buttigieg S, Tomaselli G. Defining delayed discharges of inpatients and their impact in acute hospital care: a scoping review. International Journal of Health Policy and Management. 2022;11(2):103.
- Rojas-García A, Turner S, Pizzo E. Impact and experiences of delayed discharge: A mixed-studies systematic review. Health Expectations. 2018;21(1):41-56. doi:10.1111/hex.12619
- Beck M, Okerblom D, Kumar A. Lean intervention improves patient discharge times, improves emergency department throughput and reduces congestion. Hosp Pract (1995). 2016;44(5):252-9. doi:10.1080/21548331.2016.1254559
- Orewa G, Feldman S, Hearld K. Using accountable care teams to improve timely discharge: a pilot study. Quality Management in Health Care. 2022;31(1):22-7. doi:10.1097/QMH.0000000000000320
- Zimmerman M, Benjamin I, Tirpak J, et al.. Patient satisfaction with partial hospital telehealth treatment during the COVID-19 pandemic: Comparison to in-person treatment. Psychiatry Research. 2021;301:113966.
- Adams L, Lester S, Hoon E. Patient satisfaction and acceptability with telehealth at specialist medical outpatient clinics during the COVID-19 pandemic in Australia. Internal Medicine Journal. 2021;51(7):1028-37. doi:10.1111/imj.15205
- Haidar S, Vazquez R, Medic G. Impact of surgical complications on hospital costs and revenues: retrospective database study of Medicare claims. J Comp Eff Res. 2023;12(7):e230080.
- Bentz J, Brundisini F, MacDougall D. Perspectives and Experiences Regarding the Impacts of Emergency Department Overcrowding: A Rapid Qualitative Review. Canadian Journal of Health Technologies. 2023;3(9).
- Shepperd S, Lannin N, Clemson L. Discharge planning from hospital to home. Cochrane database of systematic reviews. 2013:CD000313.
- Khanna S, Sier D, Boyle J. Discharge timeliness and its impact on hospital crowding and emergency department flow performance. Emerg Med Australas. 2016;28(2):164-70. doi:10.1111/1742-6723.12543
- Kennedy K, Orewa G, Hall A. From pandemic to endemic: A comparison of first, second, and third waves of COVID-19 for applicability in communicable disease management. Journal of Hospital Administration. 2022;11(2):1-7. doi:10.5430/jha.v11n2p1
 This work is licensed under a
This work is licensed under a 