1.Introduction
Nowadays, there are more and more women in medicine, which is already evident in medical faculties, where the number of male students is steadily decreasing. The same is true in the workplace, in hospital centres, and even in health clinics. In the Republic of Croatia, which has fewer than 4 million inhabitants and more deaths than births, the government has decided to implement incentive measures to improve the demographic situation of the country. This, however, does not favor hospital management, which is struggling to find healthcare personnel to maintain the operations of its institutions. After a young resident “discovered” the Regulation on the Rights to Maternity Leave for Pregnant Workers,[1] which has been in place since 2011, a “wave” of young female healthcare workers seeking such leave was initiated, in both justified and unjustified cases. It is true that hospitals operate in shifts, with extended working hours and night shifts, which can negatively affect pregnancy in various ways.[2,3] Premature births, miscarriages, low birth weight, stillbirths, preeclampsia, and eclampsia have been described. On the other hand, such work brings significant financial benefits, especially the pay for night shifts and overtime.[4] Shift work and disruption of sleep patterns can lead to gestational diabetes mellitus (GDM) and spontaneous miscarriages.[5,6] In general, considering the pregnancy outcomes and work conditions, female healthcare workers and laboratory staff are most concerned due to exposure to solvents, anaesthetic gases, formaldehyde, and ionizing radiation.[7] Nurses are concerned about their pregnancies due to exposure to fetotoxic and teratogenic effects on various work sites.[8] The more risk factors present in the workplace, the greater the tendency toward absenteeism.[9]
This case presents the problems of increased pressure from pregnant healthcare workers on the management of the Clinical Hospital Centre Rijeka to grant sick leave, which is paid at 100% of the salary, as is the case for professional illnesses and work-related injuries.
2.Examinees and methods
The Clinical Hospital Centre Rijeka employs around 3,500 staff, of whom 81% are women. Young women, with an average age of 31 (range 31-41), increasingly request 100% paid sick leave due to pregnancy, most often in the 8th week of pregnancy (range 5-25), attaching gynecologist reports recommending rest. Annually, nearly 3% of employed women request such sick leave up to maternity leave. The proposal for sick leave is made by the occupational medicine department at the pregnant worker’s request, along with the gynecologist’s report. The data were collected over the past year, during visits of pregnant healthcare workers to the OM unit while seeking for sick leave.
3.Results
The total number of approved sick leaves due to pregnancy varies up to 3% of the total number of employees. Since these are 100% paid sick leaves, with a steady increase in trend, this represents a significant cost for the hospital centre. In addition to the financial cost, it leads to a shortage of already insufficient healthcare personnel, potentially resulting in the closure of certain departments. There is no a statistically significant difference (
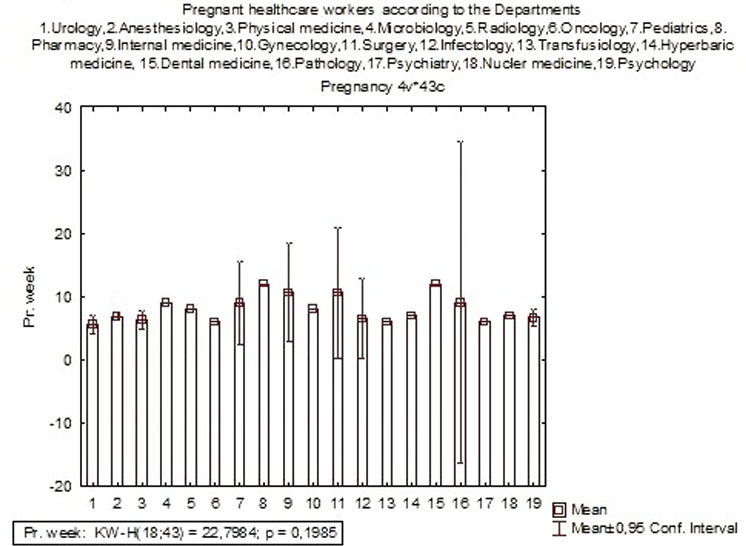
Figure 1.
Pregnant healthcare workers in weeks of pregnancy according to Departments in the Clinical Hospital Centre Rijeka
4.Discussion
When discussing ionizing radiation, medical workers are the most exposed. Low doses of radiation in female healthcare workers can lead to low birth weight, spontaneous miscarriages, and stillbirths. Radiation has a teratogenic effect, in addition to its already proven carcinogenic effects.[10] A similar situation exists with occupational exposure to anti-cancer drugs, or cytostatics.[11] Despite protective measures, cisplatin and cyclophosphamide have been found in the urine of exposed nurses, indicating that there is no absolute protection for exposed healthcare workers. Therefore, granting sick leave to pregnant healthcare workers who work in areas of ionizing radiation and with cytostatics is justified. However, there are cases where some doctors continue working in radiation zones during pregnancy, even in diagnostic radiology positions, with enhanced protective measures and avoidance of fluoroscopic X-ray tubes.[12] Some interventional radiologists also continue working during pregnancy in radiation zones.[13] The well-known saying is “The more you know about radiation, the less you fear it.”
Similarly, for female healthcare workers exposed to anaesthetic gases, it is also justified to grant sick leave, as it is for staff in infectious diseases clinics, neurology, and physical medicine, where they handle immobile and severely immobile patients and come into contact with blood and secretions.
The decision depends on each case. In any case, if the pregnant worker is assessed as fit for work, and the employer cannot find a suitable temporary position, the worker can take “ordinary sick leave” through the Croatian Health Insurance Fund, paid at around 70% of the regular salary. The occupational medicine specialist must be very cautious, especially during the first employment, to prevent exploitation of the healthcare system. There have been cases where employees are hired, and after just a few days of work, they request sick leave due to pregnancy.
The Republic of Croatia became the 28th member of the EU in 2013. The standard of healthcare is satisfactory, especially in cities and larger towns. Healthcare is managed by the Ministry of Health, which oversees the national health development strategy through the Croatian Health Insurance Fund. The Fund is financed by employed citizens, employers, and partly from EU funds. Mandatory health insurance provides insured persons with rights and obligations under such insurance, based on the principles of reciprocity, solidarity, and equality, as defined by Directive 2011/24/EU. This also includes rights in cases of work-related injuries and occupational diseases. Insured persons include policyholders, children under the age of 18, family members of the insured, and primarily individuals employed in Croatia .[14] Article 19, item 4 of the Law on Mandatory Health Insurance regulates the protection of women in relation to pregnancy monitoring and childbirth. Article 39 governs temporary incapacity due to illness and pregnancy complications. This means that in cases of pregnancy complications, women are automatically put on sick leave covered by the Fund, based on the referral of a gynaecologist and a general practitioner. In occupational medicine, we handle regular pregnancies depending on the type of job and working conditions. If the conditions are unfavourable, a healthy pregnant woman may be reassigned to another position, usually administrative work. If she refuses reassignment or continues to fear for her health and the health of her unborn child without valid reason, she is still entitled to “regular” sick leave, paid at 70%, ensuring she is financially supported.
In conclusion, if a pregnant worker fears any health consequences, there is an option, albeit with slightly lower income.
There are many cases where sick leave should be granted to pregnant women, but a critical and selective approach is necessary, as there are many requests for unjustified sick leave from healthcare workers who are not in positions with special working conditions.
It is clear that shift work and weekend work are inherently demanding, placing a significant psychophysical burden all healthcare workers. Additionally, pregnant women are in a particularly sensitive condition, requiring more frequent meals, experiencing fatigue sooner than regular workers, etc. These demands are consistent across all departments, which explains why there is no statistical difference between departments in terms of requests for sick leave. Pregnant workers that are reassigned to other workplaces with minimal potential hazards continue to work safely, with no adverse outcomes for them or their unborn child. On the contrary, if any harm had occurred, they would have the legal right to immediately sue both the medical specialist in Occupational Medicine as well as their employer – the Clinical Hospital Centre Rijeka. However, to date, no such incidents have been reported for pregnant workers and their fetuses, which suggests that the OM specialists have consistently made accurate workplace assessments. In the Republic of Croatia, pregnant women are protected under legislation, specifically the Rulebook on Conditions and Procedures for Exercising Rights to Breastfeeding Breaks and Leave for Pregnant Women, and with the Law on Mandatory Health Insurance.
The duty of the OM specialist is twofold - on one side, to protect the pregnant worker, i.e., to correctly assess that the workplace poses no risk for mother and fetus during pregnancy, and on the other side, to protect the institution, i.e., the Hospital, especially in environments where the majority of employed staff are women. In contrary, the hospital can risk severe operations problems due to the lack of employees.
With this critical and selective approach, occupational medicine, in collaboration with hospital management, can preserve hospital resources and operational capacity while safeguarding and monitoring the health and safety of pregnant workers.
Funding
The author has used his own funds to gather all the data and pay to improve personally written english text for the Journal.
Conflicts of Interest Disclosure
The author declares there is no conflicts of interest.
Informed consent
Written consent was obtained.
Ethical statement
The paper was written according to the Helsinki Declaration, no names or any personal information were not revealed and there is no possibility to connect the text with any of the female workers.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The author has in possession all the pregnant workers written search during seeking the maternal sick-leave.
Data sharing statement
The published data in Open Access are automatically free for scientific and educational sharing.
Acknowledgements
I wish to thank the professor Ana Kovačević who checked and improved the English text.
References
- Book of Rules on the Right to Sick Leave for Pregnant Workers. People’s Gazette. 2011:112.
- Cai C, Vandermeer B, Khurana R. The impact of occupational shift work and working hours during pregnancy on health outcomes: a systematic review and meta-analysis. Am J Obstet Gynecol. 2019;221(6):563-576. PMID:31276631 doi:10.1016/j.ajog.2019.06.051
- Kader M, Bigert C, Anderson T. Shift and night work during pregnancy and preterm birth — a cohort study of Swedish healthcare employees. Int J Epidemiol. 2022;50(6):1864-1874. PMID:34999871 doi:10.1093/ije/dyab135
- Booker L, Fitzgerald J, Mills J. Sleep and fatigue management strategies: How nurses, midwives, and paramedics cope with shift work schedules. Nurs Open. 2014;11(1):e2099. PMID:38268269 doi:10.1002/nop2.2099
- Wallace D, Reid K, Grobman W. Associations between evening shift work, irregular sleep timing, and gestational diabetes. Sleep. 2023;46(4):zsac297. PMID:36477807 doi:10.1093/sleep/zsac297
- Begtrup L, Specht I, Hammer P. Night work and miscarriage: a Danish nationwide register-based cohort study. Occup Environ Med. 2019;76(5):302-308. PMID:30910992 doi:10.1136/oemed-2018-105592
- Grajewski B, Rocheleau C, Lawson C. Will my work affect my pregnancy. Am J Obstet Gynecol. 2016;214(5):597-602. PMID:26976559 doi:10.1016/j.ajog.2016.03.005
- Alex M. Occupational hazards for pregnant nurses. Am J Nurs. 2011;111(1):28-37. PMID:21191230 doi:10.1097/01.NAJ.0000393056.01687.40
- Sejbäck C, Pedersen J, Schlünssen V. The influence of multiple occupational exposures on pregnancy-related work absence. Scand J Environ Health. 2020;46(1):60-68. PMID:31247116 doi:10.5271/sjweh.3840
- Frangione B, Hinton P, Villeneuve P. Low-dose ionizing radiation and adverse birth outcomes: a systematic review and meta-analysis. Int Arch Occup Environ Health. 2023;96(1):77-92. PMID:35913560 doi:10.1007/s00420-022-01911-2
- Sorsa M, Hemminki K, Vainio H. Occupational exposure to anticancer drugs-potential and real hazards. Mutat Res. 1985;154(2):135-49. PMID:3929080 doi:10.1016/0165-1110(85)90024-7
- Marx M. Baby on board: Managing occupational radiation exposure during pregnancy. Tech Vasc Interv Radiol. 2018;21(1):32-36. PMID:29471998 doi:10.1053/j.tvir.2017.12.007
- Ghatann C, Fasciotto M, Pjacobsen J. Occupational radiation exposure during pregnancy: A survey of attitudes and practices among interventional radiologists. J Vasc Interv Radiol. 2016;27(7):1013-1020.e3. PMID:27236211 doi:10.1016/j.jvir.2016.03.040
- The Law on Mandatory Health Insurance in the Republic of Croatia. People’s Gazette. 2013:80.
 This work is licensed under a
This work is licensed under a 