1.Introduction
Healthcare delivery is a complex and dynamic process that requires the coordinated input of professionals from diverse disciplines. No single cadre of health workers, irrespective of expertise, can meet the holistic needs of patients in isolation. Physicians provide diagnostic acumen and therapeutic interventions, pharmacists ensure the safe and effective use of medicines, nurses deliver round-the-clock patient monitoring and support, while laboratory scientists generate the investigative data required for clinical decision-making. Allied health professionals such as physiotherapists, radiographers, nutritionists, and administrators further enrich the care continuum. Beyond these clinical roles, facility staff including cleaners, porters, and security personnel contribute significantly to the smooth functioning of hospitals, showing that effective patient care is inherently interdependent. The framework that ensures these diverse inputs are integrated towards optimal outcomes is interprofessional collaboration (IPC).[1, 2, 3, 4]
1.1Conceptual framework
This study is anchored on the Interprofessional Collaborative Practice Framework proposed by the World Health Organization,[5] which emphasizes teamwork, communication, role clarification, and shared decision-making as key determinants of effective IPC. The framework posits that when healthcare professionals from diverse disciplines work together with mutual respect and defined roles, patient outcomes and system efficiency improve. In the Nigerian context, contextual factors such as leadership style, institutional culture, and professional hierarchies influence the extent of collaboration.[6, 7] The conceptual model for this study integrates individual-level variables (knowledge, attitude, and communication skills) and organizational-level variables (leadership support, teamwork culture, and policy environment) as predictors of IPC effectiveness. Improved IPC is expected to lead to enhanced patient care quality, reduced conflict, and improved professional satisfaction among healthcare workers in Nigerian health institutions.
1.2Knowledge gaps
Despite increasing global evidence supporting IPC, significant knowledge gaps persist within the Nigerian healthcare system. First, most Nigerian studies have focused on interprofessional conflict and rivalry rather than on the determinants of effective collaboration or its impact on patient outcomes.[6, 7] Second, there is limited empirical data on how institutional culture, leadership support, and professional education influence IPC practices in Nigerian hospitals.[8, 9] Third, while international studies emphasize the role of interprofessional education (IPE) in promoting teamwork,[10, 11] few Nigerian institutions have implemented or evaluated such initiatives. Furthermore, comparative analyses between Nigerian and global IPC models are scarce, leaving a contextual gap in adapting international best practices to local realities. This study aims to bridge these gaps by assessing factors influencing IPC among healthcare professionals in Nigeria.
IPC has become a central component of modern healthcare systems, promoting teamwork among professionals from diverse disciplines to enhance patient outcomes. Globally, IPC has been associated with improved quality of care, patient safety, and reduced medical errors.[12] The World Health Organization advocates IPC as a strategy for achieving universal health coverage through coordinated and patient-centred care.[13] In high-income countries, structured team models and IPE have improved chronic disease management and continuity of care.[14, 15]
In Nigeria, however, IPC faces multiple challenges. Studies reveal that poor communication, professional rivalry, and hierarchical barriers often hinder effective teamwork.[6, 7] Mohammed et al. identified unclear role boundaries and leadership failures as contributors to recurrent inter-professional conflicts, which undermine healthcare efficiency.[6] Despite these constraints, Nigerian healthcare workers increasingly acknowledge the value of collaboration. Opele reported that clinical personnel in tertiary hospitals view IPC as vital for knowledge exchange and improved decision-making.[8] Likewise, Halilu et al. demonstrated that IPC enhanced workflow coordination in northern Nigerian hospitals, though structural limitations persisted.[9] Among pharmacy professionals, Showande and Ibirongbe found positive attitudes toward interprofessional practice but noted limited institutional support and lack of formal IPE exposure.[16]
International evidence corroborates that IPE is a key enabler of sustainable IPC. Saragih et al. and Jiang et al. showed that IPE interventions strengthen communication, teamwork competence, and shared accountability among health professionals. Nevertheless, contextual factors such as organizational culture and policy frameworks determine success.[10, 11] Compared with global advances, Nigeria’s IPC landscape remains constrained by systemic and educational deficiencies.
Overall, existing literature affirms that IPC improves patient safety and professional satisfaction when adequately supported. Strengthening Nigeria’s health system will require embedding IPE, clarifying professional roles, and institutionalizing collaborative care policies that mirror successful global models.
1.3Importance of interprofessional collaboration
IPC is widely recognized as the gold standard for effective healthcare practice. It is defined as the process whereby multiple health workers from different professional backgrounds work together with patients, families, caregivers, and communities to deliver the highest quality of care.[17] Evidence consistently demonstrates that strong IPC improves efficiency, reduces duplication of services, enhances patient safety, and leads to better clinical outcomes.[18] Collaboration has been shown to optimize medication management, minimize preventable adverse drug reactions, reduce hospital-acquired complications, and lower morbidity and mortality rates.[19] In addition to patient benefits, IPC promotes cost-effectiveness, ensuring more sustainable use of scarce healthcare resources.[20]
Furthermore, IPC contributes to workforce well-being by fostering supportive environments where professionals feel valued. Studies reveal that effective collaboration reduces stress, burnout, and turnover while increasing job satisfaction and organizational loyalty.[21, 22, 23] It also enhances opportunities for interprofessional learning and reflective practice, leading to continuous professional development.[24]
Given these benefits, IPC has been cited as a key strategy for healthcare reform globally, with increasing calls to institutionalize collaborative approaches within health systems.[25]
1.4Core elements of effective interprofessional collaboration
The effectiveness of IPC depends on several core components: role clarity, trust and confidence, conflict resolution, collaborative leadership, and resilience in the face of adversity.[26] Role clarity ensures that each professional understands their unique contributions to patient care while respecting the input of others. When roles are well defined, teams report higher performance, greater job satisfaction, reduced stress, and enhanced organizational efficiency.[21, 27] Conversely, ambiguity leads to duplication, professional conflict, and inefficiency.
Trust and confidence are the foundation of teamwork. Trust develops gradually through personal contact, open communication, patient-centered approaches, and organizational cultures that foster fairness and respect.[22, 28] Without trust, interprofessional relationships are fragile, and collaboration quickly deteriorates.
Managing professional differences is another key element. Healthcare teams are composed of individuals with diverse training, perspectives, and personalities, and it is inevitable that disagreements arise. Effective teams transform this diversity into an asset, leveraging multiple viewpoints to stimulate innovation and problem solving.[29] Emotional intelligence, maturity, and mutual respect are critical for navigating these differences constructively.
Collaborative leadership emphasizes shared responsibility rather than hierarchical dominance. In this model, leadership is dispersed across the team, enabling collective decision-making and shared accountability. This approach fosters innovation, strengthens professional practice, and supports staff well-being.[30] Collaborative leadership has been described as encompassing resource stewardship, boundary-spanning across disciplines, and a culture of mutual respect.
Finally, resilience in adversity is vital. Health professionals often confront challenges such as resource scarcity, complex patients, or staff shortages. In such situations, collaboration becomes more critical than ever. Teams that remain united under pressure, rather than resorting to blame-shifting, demonstrate the integrity necessary for effective patient-centered care.[31]
1.5Barriers to interprofessional collaboration
Despite its recognized importance, IPC faces several barriers. A persistent challenge is professional dominance, particularly within hierarchical systems where physicians traditionally occupy the apex of authority.[32] This often breeds resentment among nurses, pharmacists, and allied professionals who feel undervalued despite their critical contributions. Conversely, doctors may resist perceived encroachments on their autonomy. Such tensions can escalate in settings where roles overlap, as increasing specialization blurs traditional professional boundaries.[33]
Communication breakdowns are another major impediment. Ineffective communication leads to misunderstandings, duplication of efforts, and medical errors. Moreover, lack of mutual respect and limited understanding of other professionals’ roles further undermine collaboration.[34]
In addition, healthcare systems often reinforce siloed practices through education, policy, and organizational structures. For example, professional training programs frequently emphasize discipline-specific competencies without adequate exposure to IPE.[26] This results in graduates who are clinically competent within their fields but ill-prepared for teamwork in complex healthcare environments.
Workforce pressures also contribute significantly. High workload, staff shortages, inadequate remuneration, and migration of health workers—often referred to as the “Japa syndrome” in Nigeria—erode morale and reduce opportunities for meaningful collaboration.[25] Under such conditions, professionals may prioritize survival strategies over teamwork.
1.6Rationale for the study
The health of a nation is inseparable from the strength of its healthcare system, and effective collaboration among professionals is a cornerstone of this strength. Poor IPC undermines patient safety, increases errors, and wastes scarce resources, outcomes that Nigeria, with its fragile health system, can ill afford. The Federal Medical Centre, Owo, Ondo State, provides an important case study for examining IPC because it is a referral facility serving diverse patient populations and employing professionals across multiple disciplines.
Understanding the perceptions and practices of healthcare workers regarding IPC in this setting is essential for identifying strengths, weaknesses, and opportunities for intervention. Such insights can guide hospital administrators, policymakers, and educators in developing strategies to strengthen collaboration, improve patient outcomes, and enhance the work environment.
In summary, IPC is indispensable for effective healthcare delivery, offering benefits that extend from improved patient safety and clinical outcomes to enhanced professional satisfaction and system efficiency. However, barriers such as professional dominance, poor communication, and systemic challenges continue to limit its full realization, particularly in Nigeria. Addressing these challenges requires deliberate strategies, including IPE, supportive leadership, and policies that foster equity and mutual respect among healthcare workers.
This study therefore seeks to assess the perceptions and practices of IPC among healthcare professionals at the Federal Medical Centre, Owo, Ondo State, Nigeria, thereby contributing evidence that can inform strategies for strengthening teamwork in the Nigerian healthcare system.
2.Methods
2.1Study design
This study adopted a descriptive cross-sectional design to assess IPC among healthcare professionals at the Federal Medical Centre, Owo, Ondo State, Nigeria. The design was chosen because it enables the researcher to collect data from diverse professional groups at a single point in time, providing a snapshot of prevailing attitudes, perceptions, and practices regarding collaboration within the healthcare team.[12] A cross-sectional design is also suitable for identifying patterns and associations among variables without manipulating the study environment.[15]
2.2Study setting
The study was conducted at FMC Owo, a tertiary healthcare institution serving as a referral center for Ondo State and neighboring communities. The hospital has a multidisciplinary workforce comprising doctors, nurses, pharmacists, physiotherapists, laboratory scientists, administrators, and allied health professionals, providing an ideal setting for examining IPC in a real-world healthcare context.
2.3Study population
The target population included all categories of healthcare professionals employed at FMC Owo as of January 2025. These included medical doctors, pharmacists, nurses, physiotherapists, medical laboratory scientists, administrators, and other allied healthcare personnel actively engaged in patient care or hospital administration.
2.4Sample size and sampling technique
The final sample size consisted of 185 participants, drawn from the various professional groups within the hospital. To ensure representativeness, a stratified random sampling technique was employed. Each professional category constituted a stratum, from which a proportionate random sample (approximately 10% of each group) was selected.
2.5Justification for the sampling technique
Stratified random sampling was chosen for several reasons:
1. Heterogeneity of the Population: The healthcare workforce at FMC Owo comprises distinct professional subgroups with varying roles, responsibilities, and hierarchical structures. Stratification ensures that all cadres are proportionally represented in the sample, minimizing sampling bias and improving the generalizability of findings.[10]
2. Comparative Analysis: This technique enables meaningful comparisons between professional groups (e.g., doctors vs. nurses or pharmacists vs. administrators) regarding their level of collaboration, trust, and communication.
3. Precision and Reliability: By reducing sampling error within each stratum, the method increases statistical precision and enhances reliability of estimates compared with simple random sampling.[15]
2.6Data collection instrument
Data were collected using a pretested, structured Interprofessional Collaboration Scale (ICS) Questionnaire, which assessed five key dimensions of IPC: role clarity, ability to overcome personal differences, trust and confidence, collective leadership, and ability to overcome adversity. Responses were rated on a five-point Likert scale ranging from strongly disagree (1) to strongly agree (5). The questionnaire was adapted to the Nigerian healthcare context and reviewed by experts in health management and behavioral sciences to ensure face and content validity.
2.7Data collection procedure
Trained research assistants from various professional backgrounds distributed the questionnaires to participants during work hours. The principal investigator supervised the process to ensure consistency and adherence to ethical standards. To enrich the quantitative findings, semi-structured interviews were conducted with selected participants to explore their experiences and perceptions of IPC in greater depth.
2.8Data analysis
Completed questionnaires were checked for completeness and coded into statistical software (SPSS version 22) for analysis. Descriptive statistics such as means, standard deviations, frequencies, and percentages were used to summarize data. Composite IPC scores were calculated for each respondent, and comparisons across professional groups were conducted using appropriate ANOVA. To ensure accuracy and reliability, the data collected were carefully validated through multiple processes. First, the questionnaire was pretested among 20 healthcare professionals from a similar tertiary hospital to identify ambiguous or poorly worded items, and necessary adjustments were made. Expert review by senior academics and clinical supervisors in health management ensured content and face validity. During data entry, double-entry verification was employed to minimize transcription errors. Internal consistency of the instrument was assessed using Cronbach’s alpha, with a threshold value of 0.70 considered acceptable.[35] Furthermore, random checks and cross-verification of responses were performed to detect missing or inconsistent data, ensuring that only complete and valid responses were included in the final analysis.
2.9Ethical considerations
Ethical approval was obtained from the Research and Ethics Committee of FMC Owo (Approval No: FMCOWO/HREC/2024/134; Reference No: NHREC/FMCOWO-HREC/03/01/2024). Informed consent was obtained from all participants, who were assured of confidentiality, anonymity, and voluntary participation with the right to withdraw at any time without penalty. The study upheld the ethical principles of respect, beneficence, and justice throughout.
3.Results
3.1Study population demographics
The study included a total of 185 participants who completed the survey, drawn from a larger staff pool across seven professional categories: Nurses (
Table 1 summarizes the demographic distribution of the 185 respondents across seven professional groups. It presents gender, marital status, age categories, years of service, and specialization levels. The majority of participants were aged 20–39 years (77.3%) with a slight female predominance (61.1%). Most respondents had less than 10 years of service (65%), and only 15.1% were specialists, reflecting the impact of workforce migration. Nurses were predominantly female (91.2%), while laboratory science was male-dominated (87.5%).
| 322 | 201 | 52 | 45 | 73 | 347 | 430 | |
| Total (%) | |||||||
| 185 (100) | 34 (18.38) | 21 (11.3) | 21 (11.3) | 20 (10.8) | 8 (4.32) | 37 (20) | 44 (23.7) |
| 157 (84.86) | 27 (74.41) | 14 (66.6) | 19 (90.4) | 13 (65.0) | 5 (62.5) | 37 (100) | 42 (95.45) |
| 28 (15.14) | 7 (20.59) | 7 (33.33) | 2 (9.52) | 7 (35.0) | 3 (37.5) | 0 (0) | 2 (4.55) |
| Male 72 (38.92) | 3 (8.82) | 11 (52.3) | 10 (47.6) | 11 (55.0) | 7 (87.5) | 15 (40.5) | 15 (34.0) |
| Female 113 (61.08) | 31 (91.18) | 10 (47.6) | 11 (52.3) | 9 (45.0) | 1 (12.5) | 22 (59.4) | 29 (65.9) |
| Single 90 (48.65) | 20 (58.8) | 6 (28.6) | 5 (23.8) | 7 (35) | 4 (50) | 7 (18.9) | 22 (50) |
| Married 95 (51.35) | 14 (41.2) | 15 (71.4) | 16 (76.2) | 13 (65) | 4 (50) | 30 (81.1) | 22 (50) |
| 20-39, 143 (77.3) | 25 (73.5) | 20 (95.2) | 19 (90.5) | 18 (90) | 7 (87.5) | 20 (54.1) | 34 (77.3) |
| 40-59, 40 (21.62) | 9 (26.5) | 1 (4.8) | 2 (9.5) | 2 (9.5) | 1 (12.5) | 15 (40.5) | 10 (22.7) |
| > 60, 2 (1.08) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (5.4) | 0 (0) |
| < 10, 120 (65) | 22 (64.8) | 17 (81) | 18 (85.7) | 17 (85) | 5 (62.5) | 18 (48.6) | 23 (52.3) |
| 10-20, 35 (18.8) | 6 (17.6) | 2 (9.5) | 2 (9.5) | 0 (0) | 2 (25) | 6 (16.2) | 17 (38.6) |
| > 20, 30 (16.2) | 6 (17.6) | 2 (9.5) | 1 (4.8) | 3 (15) | 1 (12.5) | 13 (35.2) | 4 (9.1) |
Table 2 presents mean scores for the five domains of IPC (role clarity, personal differences, trust and confidence, collective leadership, and overcoming adversity) across professions. Doctors, nurses, and pharmacists consistently reported higher scores across all domains, while administrators and the “others” category demonstrated the lowest mean scores.
| Administrator | 3.61 (0.97) | 3.44 (1.19) | 3.64 (1.13) | 3.74 (1.08) | 3.89 (1.20) |
| Doctor | 4.40 (0.66) | 4.45 (0.73) | 4.45 (0.72) | 4.37 (0.73) | 4.25 (0.89) |
| Lab Scientist | 3.91 (0.85) | 3.91 (0.99) | 3.92 (1.02) | 3.78 (0.94) | 3.90 (1.10) |
| Nurse | 4.33 (0.66) | 4.35 (0.81) | 4.34 (0.74) | 3.99 (0.84) | 4.07 (1.00) |
| Others | 3.12 (1.16) | 3.16 (1.29) | 3.08 (1.28) | 3.13 (1.25) | 3.33 (1.32) |
| Pharmacist | 4.07 (0.78) | 4.07 (0.93) | 4.22 (0.82) | 3.93 (0.87) | 4.05 (0.96) |
| Physiotherapist | 3.79 (0.86) | 3.92 (0.99) | 4.01 (0.91) | 3.81 (0.93) | 3.96 (0.97) |
Table 3 compares how each professional group rated others on role clarity. Doctors and nurses were consistently rated highly by their peers, while administrators and “others” received lower ratings. Nurses and pharmacists rated doctors highest for role clarity, while physiotherapists rated nurses highest.
| Doctor | - | 4.37 (0.63) | 3.98 (1.28) | 3.91 (1.04) | 4.11 (0.82) | 3.52 (1.17) | 3.35 (0.63) |
| Nurse | 4.53 (0.46) | - | 4.25 (1.04) | 4.02 (0.62) | 4.16 (0.69) | 3.66 (0.96) | 3.22 (0.47) |
| Pharmacist | 4.57 (0.45) | 4.43 (0.89) | - | 3.87 (0.54) | 3.92 (1.30) | 3.56 (1.02) | 3.30 (0.53) |
| Physiotherapist | 4.50 (0.40) | 4.47 (0.73) | 4.27 (1.16) | - | 4.08 (0.73) | 3.75 (0.83) | 2.97 (0.50) |
| Lab Scientist | 3.83 (1.02) | 4.00 (1.30) | 3.92 (1.53) | 3.21 (0.87) | - | 4.08 (0.94) | 2.92 (0.64) |
| Administrator | 4.17 (0.87) | 3.95 (0.76) | 3.82 (1.08) | 3.57 (0.69) | 3.68 (0.76) | - | 2.91 (0.78) |
| Others | 4.39 (0.61) | 4.27 (0.94) | 3.82 (1.23) | 3.55 (0.77) | 3.78 (0.94) | 3.32 (1.03) | - |
Table 4 shows how professional groups evaluated each other’s ability to overcome personal differences. Doctors, nurses, and pharmacists were rated more positively, with physiotherapists giving particularly high ratings to nurses. Lower scores were observed for administrators and “others,” suggesting weaker perceptions of conflict management in these groups.
| Doctor | - | 4.20 (0.67) | 3.80 (0.89) | 3.90 (0.76) | 4.00 (0.91) | 3.50 (1.02) | 3.30 (0.82) |
| Nurse | 4.50 (0.51) | - | 4.20 (0.81) | 4.10 (0.69) | 4.20 (0.74) | 3.20 (0.93) | 3.20 (0.71) |
| Pharmacist | 4.90 (0.45) | 4.50 (0.66) | - | 4.20 (0.57) | 3.90 (0.84) | 3.30 (0.76) | 3.00 (0.64) |
| Physiotherapist | 4.60 (0.47) | 4.70 (0.50) | 4.40 (0.62) | - | 4.20 (0.78) | 3.90 (0.87) | 3.40 (0.73) |
| Lab Scientist | 4.30 (0.69) | 3.90 (0.82) | 3.50 (0.91) | 3.30 (0.88) | - | 3.50 (0.89) | 2.90 (0.70) |
| Administrator | 4.10 (0.88) | 4.00 (0.73) | 3.70 (0.94) | 3.60 (0.80) | 3.60 (0.83) | - | 3.10 (0.75) |
| Others | 4.50 (0.52) | 4.30 (0.68) | 4.00 (0.82) | 3.70 (0.77) | 3.80 (0.85) | 3.20 (0.91) | - |
Table 5 outlines trust and confidence ratings across professions. Doctors, nurses, and pharmacists again received the highest ratings, particularly from one another. Administrators and “others” consistently received lower ratings, indicating limited confidence in their roles within collaborative teams.
| Doctor | - | 4.20 (0.75) | 4.10 (0.88) | 4.00 (0.82) | 3.90 (0.91) | 3.60 (0.96) | 3.20 (0.83) |
| Nurse | 4.50 (0.58) | - | 4.40 (0.81) | 4.30 (0.79) | 4.40 (0.84) | 3.50 (0.93) | 3.00 (0.72) |
| Pharmacist | 4.60 (0.47) | 4.30 (0.73) | - | 3.90 (0.82) | 4.10 (0.79) | 3.50 (0.91) | 3.20 (0.80) |
| Physiotherapist | 4.20 (0.62) | 4.30 (0.65) | 4.30 (0.74) | - | 4.10 (0.77) | 3.80 (0.87) | 3.10 (0.78) |
| Lab Scientist | 4.20 (0.66) | 3.80 (0.71) | 3.80 (0.78) | 3.60 (0.79) | - | 3.80 (0.81) | 3.00 (0.76) |
| Administrator | 4.30 (0.70) | 4.10 (0.72) | 4.10 (0.79) | 4.00 (0.81) | 3.70 (0.85) | - | 3.00 (0.80) |
| Others | 4.50 (0.54) | 4.40 (0.66) | 4.00 (0.78) | 3.70 (0.75) | 3.60 (0.82) | 3.50 (0.88) | - |
Table 6 highlights how professions evaluated each other in terms of collaborative leadership. Doctors and nurses were rated highest, while administrators and “others” were rated lowest. Interestingly, laboratory scientists gave very high ratings to doctors on this parameter.
| Doctor | - | 3.50 (0.82) | 3.40 (0.88) | 3.30 (0.85) | 3.20 (0.81) | 3.30 (0.87) | 3.00 (0.80) |
| Nurse | 4.40 (0.66) | - | 4.20 (0.74) | 4.10 (0.72) | 4.00 (0.78) | 3.50 (0.89) | 3.00 (0.76) |
| Pharmacist | 4.50 (0.54) | 4.00 (0.69) | - | 3.80 (0.77) | 3.90 (0.80) | 3.80 (0.84) | 3.00 (0.78) |
| Physiotherapist | 4.20 (0.60) | 4.10 (0.67) | 4.10 (0.72) | - | 4.10 (0.76) | 4.00 (0.83) | 3.20 (0.79) |
| Lab Scientist | 4.90 (0.50) | 4.30 (0.65) | 3.80 (0.73) | 3.80 (0.74) | - | 3.60 (0.82) | 3.40 (0.77) |
| Administrator | 4.20 (0.63) | 3.80 (0.69) | 3.80 (0.74) | 3.70 (0.73) | 3.70 (0.78) | - | 3.40 (0.75) |
| Others | 4.40 (0.57) | 3.90 (0.66) | 3.70 (0.73) | 3.60 (0.72) | 3.60 (0.77) | 3.60 (0.81) | - |
Table 7 demonstrates how teams perceived one another’s ability to collaborate under adversity. Doctors and nurses scored highest, particularly in evaluations from peers, while administrators and “others” had the lowest ratings.
| Doctor | - | 4.00 (0.83) | 3.90 (0.88) | 4.00 (0.82) | 3.80 (0.87) | 3.70 (0.89) | 3.30 (0.80) |
| Nurse | 4.60 (0.52) | - | 4.40 (0.74) | 4.40 (0.71) | 4.40 (0.76) | 4.10 (0.81) | 3.30 (0.77) |
| Pharmacist | 4.40 (0.57) | 4.30 (0.68) | - | 3.80 (0.74) | 3.80 (0.79) | 3.70 (0.80) | 2.90 (0.71) |
| Physiotherapist | 4.10 (0.63) | 4.10 (0.67) | 4.20 (0.72) | - | 4.00 (0.75) | 3.90 (0.78) | 3.60 (0.74) |
| Lab Scientist | 4.10 (0.66) | 3.60 (0.71) | 3.80 (0.77) | 3.50 (0.73) | - | 3.70 (0.76) | 3.00 (0.72) |
| Administrator | 3.90 (0.70) | 3.70 (0.74) | 3.60 (0.78) | 3.60 (0.75) | 3.50 (0.79) | - | 3.30 (0.74) |
| Others | 4.40 (0.54) | 4.00 (0.67) | 4.00 (0.71) | 3.90 (0.70) | 3.80 (0.74) | 3.80 (0.77) | - |
3.2Overall interprofessional collaboration scores
One-way ANOVA analysis demonstrated that perceptions of IPC differed significantly across the professional groups for all five dimensions assessed (
| Role Clarity | 47.64 | < .001 |
| Personal Differences | 38.88 | < .001 |
| Trust & Confidence | 44.47 | < .001 |
| Collective Leadership | 27.59 | < .001 |
| Overcoming Adversity | 13.37 | < .001 |
Table 8 reports the results of ANOVA analyses comparing IPC domain scores across professions. Significant differences were found in all domains (
3.3Inter-professional perception (pater vs. target analysis)
Post-hoc analysis using the Games–Howell test provided critical insight into the perceived collaborative competence of specific target professions by their colleagues (see Table 9).
| Role Clarity | Doctors & Nurses > Pharmacists & Lab scientists | Others & Administrators > Physiotherapist | < .05 |
| Personal Differences | Doctor > Nurse > Pharmacists, Physiotherapists & Lab scientist | Others & Administrators | < .05 |
| Trust & Confidence | Doctors > Nurses & Pharmacists > Physiotherapists & Lab scientists | Others & Administrators | < .05 |
| Collective Leadership | Doctor > Nurses > Lab scientists & Pharmacists | Others > Administrators & Physiotherapists | < .05 |
| Overcoming Adversity | Doctor > Nurse > Pharmacists & Physiotherapists | Others & Administrators > Lab scientists | < .05 |
3.4Role clarity
In the dimension of role clarity, Doctors and Nurses were rated significantly higher than Pharmacists and Lab Scientists (
3.5Personal differences
Perceptions regarding the ease of managing Personal Differences showed a clear hierarchy, with Doctors rated significantly higher than Nurses, who in turn were rated higher than Pharmacists, Physiotherapists, and Lab Scientists (
3.6Trust and confidence
The level of Trust and Confidence reflected a similar positive bias towards the clinical professions. Doctors were rated higher than Nurses and Pharmacists, who were rated higher than Physiotherapists and Lab Scientists (
3.7Collective leadership
Perceptions of Collective Leadership were significantly higher for Doctors compared to Nurses, who were rated higher than Lab Scientists and Pharmacists (
3.8Overcoming adversity
Finally, the ability to successfully Overcome Adversity followed the established pattern, with Doctors rated significantly higher than Nurses, who were in turn rated higher than Pharmacists and Physiotherapists (
Table 9 provides pairwise comparisons of mean scores. Doctors and nurses consistently received the highest ratings across domains, while administrators and “others” were rated lowest. Pharmacists performed moderately well, while physiotherapists and laboratory scientists often occupied intermediate positions.
Figure 1 visualizes how each professional group rated others in terms of role clarity. Doctors and nurses show the strongest role clarity across ratings, while administrators and “others” demonstrate weaker clarity.
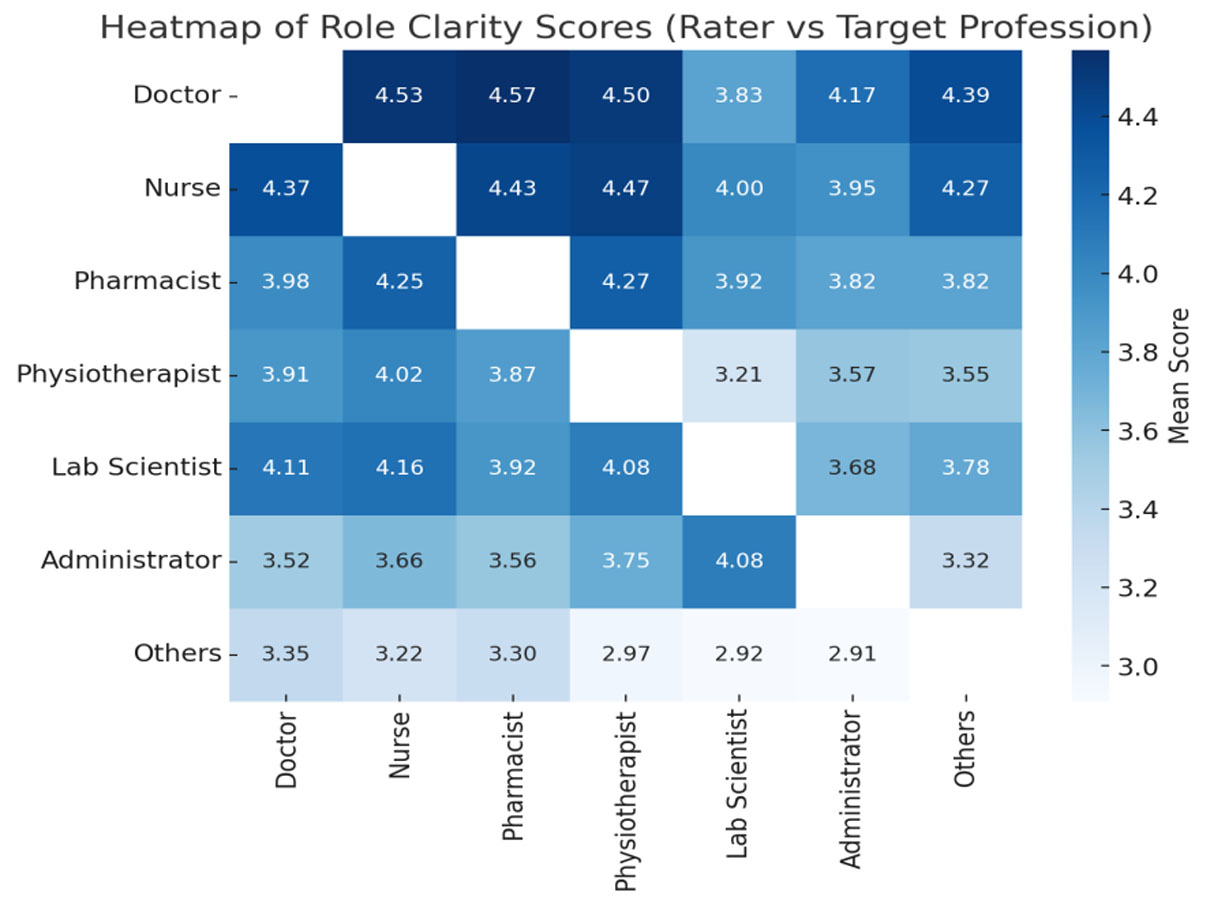
Figure 1.
Heatmap of role clarity scores of the target professionals
Figure 2 illustrates comparative ratings of how professions managed personal differences. Doctors and nurses are again perceived more positively, while administrators and “others” are less well regarded.
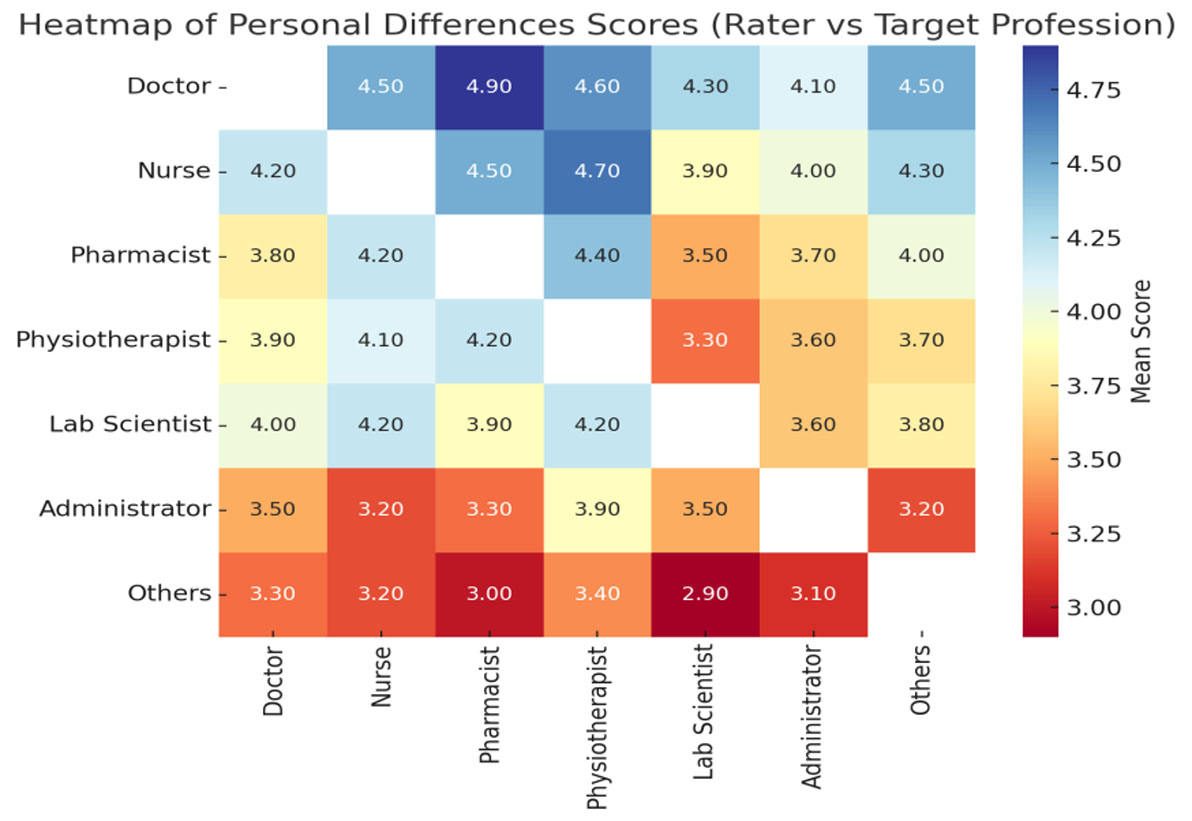
Figure 2.
Heatmap of personal difference scores of the target professionals
Figure 3 displays interprofessional perceptions of trust and confidence. The strongest trust is observed among doctors, nurses, and pharmacists, while administrators and “others” remain at the lower end of the scale.
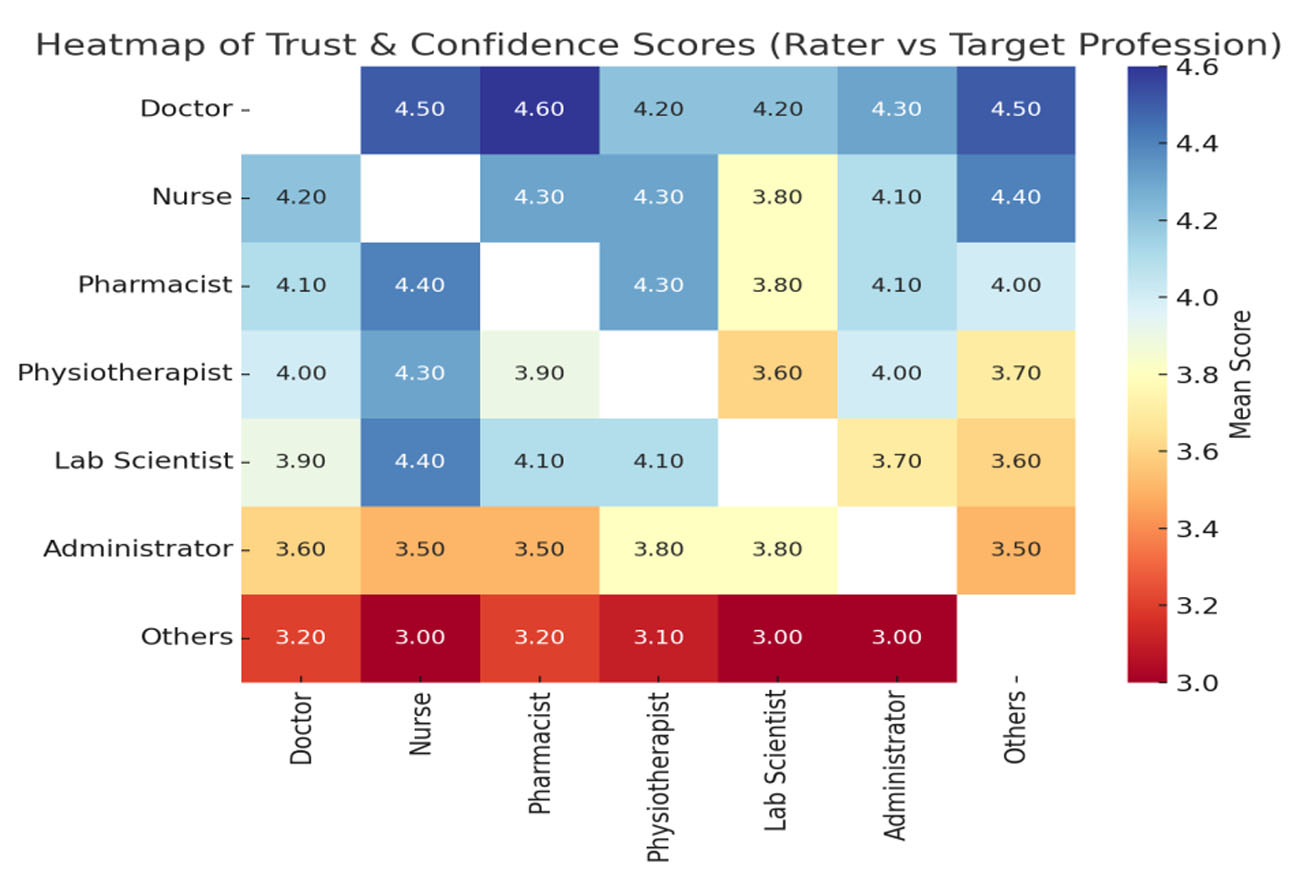
Figure 3.
Heatmap of trust and confidence scores of the target professionals
Figure 4 depicts collective leadership ratings. Doctors and nurses are consistently rated highly across professional groups, whereas administrators and “others” receive comparatively low scores.
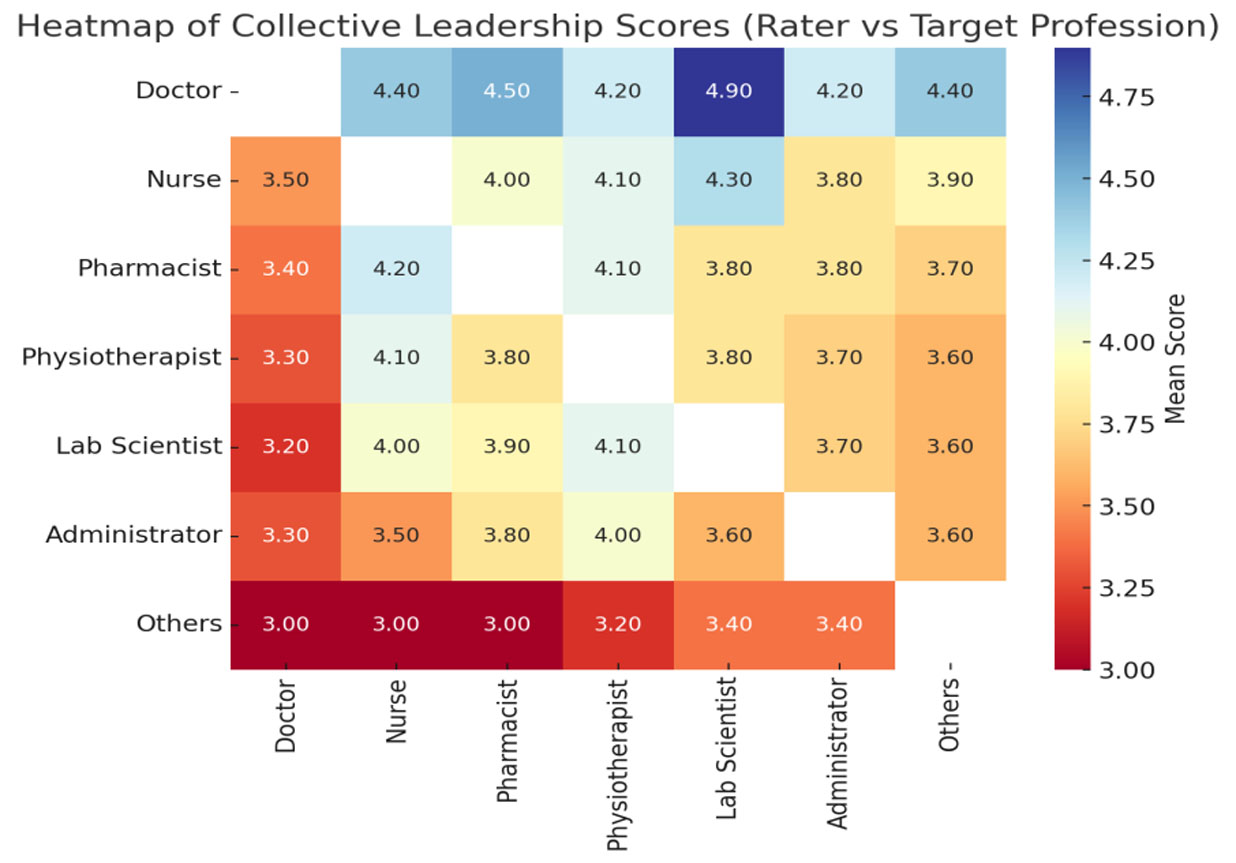
Figure 4.
Heatmap of collective leadership scores of the target professionals
Figure 5 shows ratings of how teams perform under adversity. Doctors and nurses are consistently perceived as resilient collaborators, while administrators and “others” are rated lowest across groups.
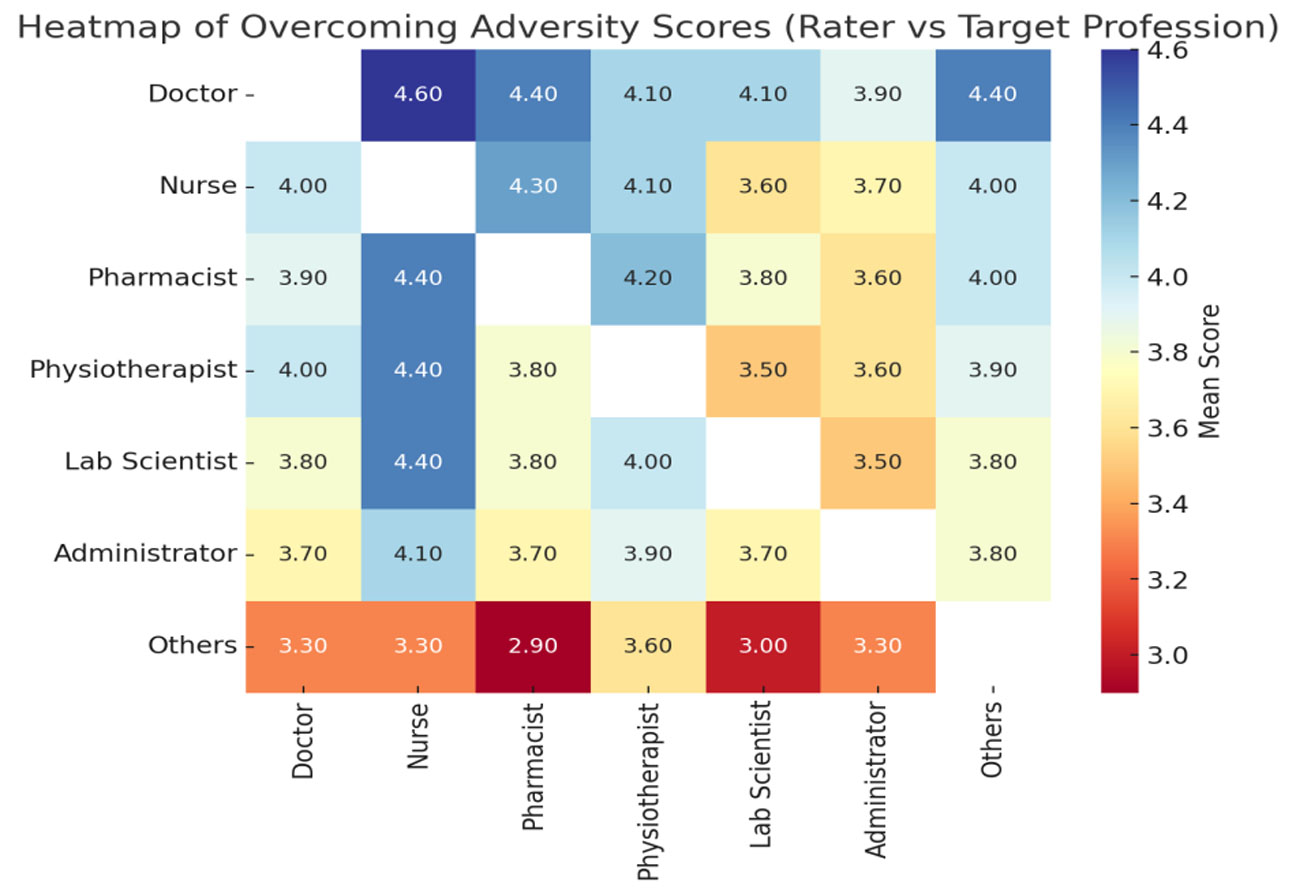
Figure 5.
Heatmap of overcoming adversity scores of the target professionals
4.Discussion
The present study examined IPC among healthcare workers at the Federal Medical Centre, Owo, Nigeria, focusing on role clarity, ability to overcome personal differences, trust and confidence, collective leadership, and capacity to overcome adversity. The findings highlight both the strengths and weaknesses of interprofessional practices within a tertiary hospital setting and provide insights into the dynamics of collaboration between different cadres of healthcare workers in Nigeria.
One of the striking demographic features of the study population was its youthfulness as seen in Table 1. More than three-quarters of respondents were between 20 and 39 years of age, with only a small minority above 60 years. This reflects the general demographic distribution of Nigeria’s workforce and the mandatory retirement age of 60 years for civil servants. It also speaks to the problem of retention within the Nigerian health sector, where high rates of emigration, the so-called “Japa syndrome” have left hospitals with younger, less experienced staff. A similar trend was noted by Ogbimi and Adebamowo in their study of Nigerian teaching hospitals, where they highlighted how instability in the health workforce weakened continuity of care and collaboration.[13] Younger workers may bring energy and innovation, but their relative lack of experience and specialization, as seen in our finding that only 15% of respondents were specialists, can limit the maturity of collaborative practice.
Gender distribution followed expected patterns. Females constituted 61% of respondents, with nursing being overwhelmingly female and laboratory science heavily male-dominated. These findings echo global trends, where nursing remains a female-dominated profession, while laboratory and biomedical sciences attract more men. Masibo and colleagues in Tanzania have similarly highlighted the strong gendered identities within health professions, which in turn shape professional relationships and collaboration.[27] While other groups such as doctors, pharmacists, and physiotherapists showed more gender balance, the persistence of gender stereotypes within nursing and laboratory sciences may reinforce hierarchical dynamics, with potential implications for interprofessional trust and respect.
The findings across the five IPC domains reinforce the entrenched hierarchy within Nigerian healthcare. Doctors rated themselves highly across all parameters and were similarly rated highly by most other groups as seen in Table 2. Nurses and pharmacists also rated themselves positively, although with slightly lower scores for collective leadership, while physiotherapists, laboratory scientists, administrators, and ancillary staff consistently scored themselves, and were scored by others lower, across all domains.
These results mirror the classic description by Stein of the “doctor–nurse game,” in which physicians occupy a dominant position in clinical decision-making, with other professionals adapting around them.[4] Although the dynamics have evolved, the centrality of doctors as leaders in Nigerian hospitals remains evident in the consistently high ratings they received in this study.
Nurses and pharmacists occupied a middle ground. They rated themselves highly in most domains and were positively evaluated by doctors, physiotherapists, and sometimes administrators. This may be due to their central roles in patient care and frequent collaboration with physicians. Gregory and Austin, in their Canadian study, found that pharmacists have gained increasing recognition as trusted collaborators in recent years, particularly in areas of medication safety and optimization.[22] Our findings suggest a similar trend, with pharmacists receiving high trust and confidence scores, though their relatively lower collective leadership scores point to the persistence of hierarchical constraints.
Physiotherapists and laboratory scientists, however, were less favorably evaluated. Their contributions, though essential, are often indirect and occur outside the immediate patient care setting, which may explain their lower visibility in interprofessional assessments. Masibo and colleagues have reported similar struggles for visibility among physiotherapists in East Africa, where their expertise is vital in rehabilitation but often undervalued within multidisciplinary teams.[27] Laboratory scientists may face even greater challenges, as their patient interactions are minimal, and their roles are often confined to diagnostic support. This limited visibility may contribute to their lower ratings in role clarity, leadership, and trust.
Administrators and other ancillary staff, grouped as “others,” were consistently rated lowest across all domains. This finding underscores a critical gap in how healthcare workers perceive the contributions of non-clinical staff to IPC. Yet, these groups are indispensable for the smooth functioning of hospitals. A system that undervalues their roles risks undermining the broader collaborative ethos that IPC demands. Elsous et al., in their study of nurse–physician collaboration in Gaza, highlighted that exclusion of ancillary staff from team processes weakens communication, coordination, and ultimately patient outcomes.[36] A similar issue is evident in the Nigerian context, where administrators and support staff may be sidelined from interprofessional dialogue.
The analysis of role clarity showed doctors and nurses enjoying the highest ratings, consistent with their clearly defined roles in patient care as seen in Table 3. This resonates with the findings of Unegbu and colleagues, who emphasized that role clarity enhances job satisfaction and organizational efficiency.[21] The ability to overcome personal differences was also strongest among doctors, while administrators and ancillary staff were rated lowest. This suggests that clinical staff are better equipped or at least perceived to be better equipped to manage interpersonal conflicts compared to administrative staff. Trust and confidence followed a similar pattern, with doctors, nurses, and pharmacists enjoying the highest ratings, underscoring the centrality of clinical professionals in shaping team trust.
Collective leadership emerged as the weakest domain across professions, with only doctors consistently rated highly as seen in Table 6. This reflects the persistence of hierarchical models of leadership in Nigeria, where decision-making authority is concentrated among physicians.
Bosch and Mansell have argued that genuine collective leadership requires dismantling these traditional hierarchies and distributing leadership across professions.[30] The challenge is particularly acute in Nigeria, where entrenched professional rivalries, union activism, and remuneration disparities reinforce existing hierarchies.
In the domain of overcoming adversity, doctors and nurses again received the highest ratings, reflecting their central roles in crisis management and direct patient care. Baggs and colleagues demonstrated in their American study that strong nurse–physician collaboration during critical care situations significantly improved patient outcomes,[32] a finding echoed here. However, the low ratings given to administrators and ancillary staff suggest that resilience under pressure is not perceived as a collective responsibility but is concentrated within clinical cadres.
Taken together, these findings illustrate a collaboration landscape characterized by strong doctor–nurse–pharmacist alliances, weaker integration of physiotherapists and laboratory scientists, and near exclusion of administrators and ancillary staff. This pattern reflects not only professional hierarchies but also systemic weaknesses in fostering inclusive collaboration. The Nigerian health system’s challenges including migration, workforce shortages, and poor investment in IPE exacerbate these dynamics. Ogbimi and Adebamowo observed that weak collaboration between doctors and nurses in Nigerian hospitals was not merely a professional problem but a systemic one, rooted in organizational structures and policy environments.[25]
Comparisons with other studies highlight both parallels and divergences. Kim’s original work on the doctor–nurse game continues to resonate in the Nigerian context, although recent studies such as Hojat et al. in the United States show evolving attitudes, with younger professionals increasingly open to shared decision-making.[26] Gregory and Austin’s work demonstrates that pharmacists can become central collaborators when systems intentionally integrate them, suggesting a path forward for Nigeria. Masibo’s East African findings and Elsous’s Palestinian findings both confirm that undervaluing certain professions leads to marginalization and weakens collaboration, patterns mirrored in this study. Finally, Baggs et al. stated that effective collaboration, particularly between doctors and nurses, is not merely a matter of professional harmony but directly tied to patient safety and outcomes.[22, 27, 32, 36]
The implications of this study are clear. First, there is an urgent need to clarify roles and responsibilities across all professional groups to strengthen collaboration. Second, IPE should be institutionalized at undergraduate and postgraduate levels to foster mutual understanding and respect among healthcare professionals. Third, collective leadership models must be actively promoted, with opportunities for nurses, pharmacists, physiotherapists, and even administrators to take leadership roles in patient care teams. Fourth, deliberate strategies are needed to build trust across professions, including joint ward rounds, interdisciplinary meetings, and cross-training opportunities. Finally, policies to stem the tide of migration and improve workforce retention are essential, as a stable and experienced workforce is more likely to engage in meaningful collaboration.
5.Conclusion
This study revealed that although doctors, nurses, and pharmacists demonstrated relatively strong levels of IPC, other professional groups, including physiotherapists, medical laboratory scientists, administrators, and ancillary staff, were less integrated into collaborative decision-making processes at Federal Medical Centre, Owo, Nigeria. The findings highlight the continued influence of professional hierarchies, limited communication across disciplines, and unequal recognition of roles within the healthcare system. These barriers hinder the realization of effective team-based care and compromise service delivery quality.
To enhance collaboration, there is an urgent need for structural reforms that promote shared leadership and inclusive teamwork, as well as educational strategies such as IPE embedded in training curricula to foster mutual respect and understanding. Additionally, organizational culture change must prioritize transparency, trust-building, and equitable participation among all cadres of healthcare workers.
Since institutional culture can strongly shape interprofessional relationships, it would be inappropriate to assume that these findings fully represent other hospitals in Nigeria or beyond.
Future studies involving multi-center participation and larger, more balanced samples are recommended to strengthen the external validity of the results and provide a broader understanding of IPC patterns across healthcare institutions.
In summary, strengthening IPC is not merely desirable; it is critical to improving healthcare outcomes, patient safety, and institutional efficiency. As evidenced in this study, achieving sustainable, patient-centered care in Nigeria and globally depends on dismantling professional silos and nurturing a collaborative culture within the healthcare workforce.
Limitations of the study
Despite its robust design and adherence to ethical standards, this study faced several limitations. First, as a single-center cross-sectional study, findings from Federal Medical Centre, Owo may not be fully generalizable to other healthcare institutions in Nigeria, especially private or primary healthcare settings with different organizational cultures and structures.[12] So, stratified random sampling technique was carefully selected to ensure that our study truly represent the opinion of the staff of FMC, Owo. Second, self-reported data obtained through questionnaires are prone to social desirability and recall bias, as participants may provide responses they consider professionally acceptable rather than reflecting their true attitudes.[15] To reduce this recall bias, a semi-structured interviews and the use of structured questionnaire (data triangulation) were conducted with selected participants in the study. Moreover, data were collected anonymously. Additionally, the unequal representation of professional groups, particularly laboratory scientists and physiotherapists, may have limited the ability to detect profession-specific variations in collaboration. Finally, the cross-sectional design restricts causal inference, preventing assessment of temporal or intervention-related changes in IPC.[10] This unequal representation of certain professions and study design type will form the basis for a multicentre study.
Authors contributions
FTO Correponding author: Conceptualized, designed the study and wrote the first draft of manustrip. Developed the statistical analysis plan and performed the statistical analyses with ATM. ATM and FTO did literature search and final manustrip write up. FAE, AYA, AKI, OOI: Questionaires administration and data collection. All authors have given final approval for the current version to be published.
Funding
No external funding was received.
Conflicts of Interest Disclosure
The authors declare they have no conflicts of interest.
Informed consent
Obtained.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Data sharing statement
The data can be requested from the corresponding author.
Acknowledgements
We acknowledged the hospital staff of Federal Medical Centre, Owo, who assisted us in data collection.
References
- Shi Y, Wang X, Chen L. The nurse-physician relationship during the COVID-19 pandemic: A mixed-methods study and model of collaborative attitudes. JMIR Form Res. 2023;7:e41729. PMID:36745499 doi:10.2196/41729
- Sculon D, Lindroth R, Christianson J. Steering patients to safer hospitals. Health Serv Res. 2008;43(5 Pt 2):1849-68. PMID:18761676 doi:10.1111/j.1475-6773.2008.00889.x
- Kim Y, Oh Y, Lee E. Impact of nurse-physician collaboration, moral distress, and professional autonomy on job satisfaction among nurses acting as physician assistants. Int J Environ Res Public Health. 2022;19(2):661-75. PMID:35055482 doi:10.3390/ijerph19020661
- Rahayu S, Prasetyo D. Does power distance in healthcare teams link to patient outcomes? Evidence from multi-disciplinary hospital teams. BMC Health Serv Res. 2024;24:83. PMID:38229081 doi:10.1186/s12913-023-10534-3
- World Health Organization (WHO). Framework for action on interprofessional education and collaborative practice. 2010. https://apps.who.int/iris/handle/10665/70185
- Mohammed E. Knowledge, causes, and experience of inter-professional conflict and rivalry among healthcare professionals in Nigeria. BMC Health Serv Res. 2022;22:320. PMID:35264179 doi:10.1186/s12913-022-07664-5
- Adigwe O, Mohammed E, Onavbavba G. Preventing and mitigating inter-professional conflict among healthcare professionals in Nigeria. J Healthc Leadersh. 2023;15:1-9. PMID:36636738 doi:10.2147/JHL.S392882
- Opele J. Inter-professional collaboration and knowledge management practices among clinical workforce in federal tertiary hospitals in Nigeria. Knowl Manag E-Learn. 2022;14(3):329-43. doi:10.34105/j.kmel.2022.14.018
- Halilu S, Maiyegun A, Aiyekomogbon J. Interprofessional collaboration amongst healthcare workers of a tertiary hospital in north-eastern Nigeria. Niger Postgrad Med J. 2024;31(2):163-9. PMID:38826020 doi:10.4103/npmj.npmj_281_23
- Saragih I, Arna Uly Tarihoran D. A systematic review and meta-analysis of outcomes of interprofessional education for healthcare students from seven countries. Nurse Educ Pract. 2023;71:103683. PMID:37433234 doi:10.1016/j.nepr.2023.103683
- Jiang Y, Cai Y, Zhang X. Interprofessional education interventions for healthcare professionals to improve patient safety: A scoping review. Med Educ Online. 2024;29(1):2391631. PMID:39188239 doi:10.1080/10872981.2024.2391631
- Wei H, Horns P, Sears S. A systematic meta-review of systematic reviews about interprofessional collaboration: facilitators, barriers, and outcomes. J Interprof Care. 2022;36(5):735-749. doi:10.1080/13561820.2021.1973975
- Bouton C, Journeaux M, Jourdain M. Interprofessional collaboration in primary care: What effect on patient health. BMC Prim Care. 2023;24:253. PMID:38031014 doi:10.1186/s12875-023-02189-0
- Grant A, Kontak J, Jeffers E. Barriers and enablers to implementing interprofessional primary care teams: a narrative review of the literature using the consolidated framework for implementation research. BMC Prim Care. 2024;25(1):25. PMID:38216867 doi:10.1186/s12875-023-02240-0
- Rawlinson C, Carron T, Arditi C. An overview of reviews on interprofessional collaboration in primary care: Effectiveness, barriers and facilitators. Int J Integr Care. 2021;21(2):32, 1-15. doi:10.5334/ijic.5589
- Showande S, Ibirongbe T. Interprofessional education and collaborative practice in Nigeria: Pharmacists’ and pharmacy students’ attitudes and perceptions. Curr Pharm Teach Learn. 2023;15(9):787-800. PMID:37482495 doi:10.1016/j.cptl.2023.07.013
- World Health Organization. Framework for action on interprofessional education and collaborative practice. 2010.
- Bosch B, Mansell H. Interprofessional collaboration in health care. Can Pharm J (Ott). 2015;148(4):176-9. PMID:26448769 doi:10.1177/1715163515588106
- Krogstad U, Hofoss D, Hjortdahl P. Doctor and nurse perception of inter-professional co-operation in hospitals. Int J Qual Health Care. 2004;16(6):491-7. PMID:15557359 doi:10.1093/intqhc/mzh082
- Sweet S, Norman I. The nurse-doctor relationship: A selective literature review. J Adv Nurs. 1995;22(1):165-70. PMID:7560525 doi:10.1046/j.1365-2648.1995.22010165.x
- Unegbu V, Ayoola O, Oduwole A. Role clarity as a determinant of job satisfaction among library personnel in South-West Nigeria. J Inf Knowl Manag. 2023;14(1):126-43. doi:10.4314/iijikm.v14i1.8
- Gregory P, Austin Z. Trust in interprofessional collaboration. Can Pharm J (Ott). 2016;149(4):236-45. PMID:27540406 doi:10.1177/1715163516647749
- Svensson R. The interplay between doctors and nurses—a negotiated order perspective. Sociol Health Illn. 1996;18(3):379-98. doi:10.1111/1467-9566.ep10934735
- Clark K. Interprofessional education and collaborative practice: Are we there yet. J Lung Health Dis. 2018;2(4):1-5. doi:10.29245/2689-999X/2017/4.1139
- Ogbimi R, Adebamowo C. Questionnaire survey of working relationships between nurses and doctors in University Teaching Hospitals in Southern Nigeria. BMC Nurs. 2006;5:2. doi:10.1186/1472-6955-5-2
- Hojat M, Nasca T, Cohen M. Attitudes toward physician-nurse collaboration: A cross-cultural study. Nurs Res. 2001;50(2):123-8. PMID:11302292 doi:10.1097/00006199-200103000-00008
- Masibo R, Kibusi S, Masika G. Gender dynamics in nursing profession: Impact on practice in Tanzania. BMC Health Serv Res. 2024;24:1179. PMID:39363160 doi:10.1186/s12913-024-11641-5
- Miller P. Nurse-physician collaboration in an intensive care unit. Am J Crit Care. 2001;10(5):341-50. PMID:11548567 doi:10.4037/ajcc2001.10.5.341
- Steinbrook R. Nursing in the crossfire. N Engl J Med. 2002;346(22):1757-66. PMID:12037165 doi:10.1056/NEJM200205303462225
- Thomas E, Sexton B, Helmreich R. Discrepant attitudes about teamwork among critical care nurses and physicians. Crit Care Med. 2003;31(3):956-9. PMID:12627011 doi:10.1097/01.CCM.0000056183.89175.76
- Adebayo A, Ilesanmi O. Collaboration between doctors and nurses in a Nigerian tertiary hospital. Int J Collaborative Soc. 2016;9(1):165.
- Baggs J, Schmitt M, Mushlin A. Association between nurse-physician collaboration and patient outcomes in ICUs. Crit Care Med. 1999;27(9):1991-8. PMID:10507630 doi:10.1097/00003246-199909000-00045
- Adebayo A, Ilesanmi O. Collaboration between doctors and nurses in a tertiary health facility in South West Nigeria: Implication for effective healthcare delivery. Int J Collaborative Soc. 2016;9(1):165.
- Thomson S. Nurse-physician collaboration: a comparison of the attitudes of nurses and physicians in the medical-surgical patient care setting. Medsurg Nurs. 2007;16(2):87-91, 104. PMID:17547265
- Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53-5. PMID:28029643 doi:10.5116/ijme.4dfb.8dfd
- Elsous A, Radwan M, Mohsen S. Nurses’ and physicians’ attitudes toward nurse-physician collaboration: A survey from Gaza Strip, Palestine. Nurs Res Pract. 2017;2017:7406278. PMID:28326194 doi:10.1155/2017/7406278
 This work is licensed under a
This work is licensed under a 