1.Introduction
Healthcare delivery organizations (HDOs) are routinely implementing mobile projects as enterprise-wide initiatives to improve operational productivity and clinical care workflows.[1,2,3,4,5,6] Deployment of shared-use mobile devices is increasing due to the workflow flexibility they offer, along with cost savings compared to individual or personal device use. Shared-use mobile devices ease and expedite information access across the facility.[1] Mobile device adoption in hospitals is also driven by an increasing number of Internet of Medical Things (IoMT) devices and applications designed to improve care effectiveness and efficiency.[2,3,4,5,6] As point-of-care opportunities and capabilities increase, HDOs need to enable real-time, rapid and secure transfer of patient data across the institutional network, where shared-use mobile devices can be deployed to increase clinical workflow efficiency, as well as clinician satisfaction.[7] With increasing clinical workflows at the bedside accessible through mobile device technology, there is growing demand for access to needed patient clinical information and care applications at the point of care delivery.[8] HDOs are therefore engaging mobile solutions to improve workflow flexibility and collaboration across the care delivery team.[2] Less costly to acquire and support than desktop workstations, shared-use mobile devices also offer potential financial savings if well managed and secure.[9]
Growth in clinician use of mobile devices has presented significant challenges in ensuring data privacy/secure access with proper user authentication, particularly when mobile devices are exchanged among different clinical users. Shared-use mobile devices can be implemented without a meaningful reduction in information security and data privacy, but doing so requires that HDOs implement and optimally manage the technology in a systematic and deliberate manner, while minimizing usability and adoption impediments.[8] Effective and seamless digital identity management are key to maintaining security and minimizing points of device exposure, and usability barriers.
This survey sought to understand HDO perceptions on shared-use mobile device adoption and management, and to identify institutional challenges and needed capabilities across four nations. Research on the adoption of shared-use mobile devices by hospitals and clinicians can help define unmet needs created by mobile workflows, and highlight the imperative to effectively and efficiently manage a fleet of mobile devices.[8, 10, 11] It is important during this adoption period to increase understanding of the issues that HDOs are encountering in expanding clinical mobility and mobile workflows. A lack of standardized, systematic operational processes and tools to manage a mobile device fleet and workflows can impede the uptake and utilization of the technology if tools do not keep pace with the implementation.[8, 10,11,12,13,14] The HDO survey reported here also sought insights regarding differences in the perceived issues and challenges across four nations that are rapidly adopting mobile devices in care delivery.
2.Methods
The overall study objective was to assess current and prospective hospital utilization of mobile devices, and enterprise-level management of a mobile device fleet in four nations, including Australia, Canada, the United Kingdom (UK) and the United States (US). Four specific areas of interest included: (1) assessment of current adoption and usage of shared-use mobile devices in HDOs; (2) exploration of the benefits of shared-use mobile devices in enhancing clinical workflows, patient care delivery, and operational efficiency; (3) identification of key challenges and barriers to effective implementation and use of shared-use mobile devices, including security, workflow integration, asset management, and user experience; and (4) establishment of a baseline for year-on-year benchmarking to track trends, adoption patterns, and evolving attitudes toward mobile device usage in healthcare. The survey also focused on the effective and efficient management of enterprise shared-use mobile devices.
An online fully de-identified, anonymous survey was administered to gather information about the perceptions, views and operational practices of healthcare information technology (IT) decision makers and clinicians regarding the current institutional status, challenges, and unmet needs in managing clinical mobile devices in their HDOs. The former group was evaluated in the screening process for knowledge of their organization’s shared mobile initiatives, and clinicians focused on chief medical officers or physician leaders with knowledge of hospital clinical informatics strategies and programs. All HDOs had to be acute care facilities. All respondents must have shared-use devices deployed at their organization. Four hundred fully completed responses were collected via online surveys across the four nations. The HDO respondent pool consisted of 242 IT decision makers and 158 clinical leaders. Eligible respondents had to work at facilities with more than 100 patient beds and at least 500 employees.
Current and expected future adoption and usage of shared-use mobile devices, perceived benefits, and clinical care, operational and security needs and challenges were evaluated. In addition, barriers to effective implementation of shared-use mobile devices were explored, with a particular emphasis on clinician access to mobile devices and through them access to clinical applications and information. Device management challenges that could potentially create operational and security issues and organizational risk were also assessed.
The survey questionnaire was 20 questions in length for either respondent type (excluding screener/profiling and routed questions), and predominantly standard questions were used (including single or multiple choice format). The survey was pre-tested, including a live field test completed with 10–15 respondents. This involved a pilot call with screenshare walking through the survey questions. Minor changes to the instrument were made based on these results, along with amendments to the online survey script. Necessary quality checks ensured that the insights from the survey were built on dependable data. These included real-time data checking and multi-factor validation across a range of metrics. The survey started with an initial soft launch which ran for one week, and was followed by a full-scale launch to respondents which continued for 2 additional weeks.
Survey responses were quantified and tabulated. Data tables in Microsoft Excel containing the complete and final data were generated. Survey data were analyzed using stratified contingency tables, and figures were generated to share the response results differentiated by nation. As such, ethical review and IRB approval were not needed or sought.
This study did not involve patients or collection of any patient data, and the survey of clinicians and healthcare IT personnel was completed on an opt-in basis where respondents explicitly agreed to have their data analyzed and published in aggregate, de-identified form. As such, a waiver of IRB approval and ethical review was not needed or sought.
3.Results
3.1Respondents
Four hundred leaders from acute care facilities with 100–1,000 or more beds were surveyed in Australia, Canada, the UK and the US. Seventy-nine percent were based at private hospitals or health systems, and the balance were in the public sector. Table 1 shows the breakdown of respondents by facility bed count.
| 100-249 beds | 39 | 10% |
| 250-499 beds | 104 | 26% |
| 500-749 beds | 92 | 23% |
| 750-999 beds | 85 | 21% |
| 1,000 or more beds | 80 | 20% |
| Total | 400 | 100% |
| Mean = 669 beds | ||
Survey respondents by nation where located were as follows: 75 (18.8%) were based in Australia; 60 (15.0%) in Canada; 125 (31.2%) in the UK; and 140 or 35% of respondents were in the US. With respect to organizational role, the respondent pool consisted of 242 (60.5%) IT decision makers and 158 (39.5%) clinical leaders.
3.2Current state of shared-use mobile device policies and practices and growth expectations
Ninety-two percent of all respondents agreed that mobile devices are essential tools in healthcare facilities. Yet only 56% overall across the four nations had fully implemented shared-use device policies and procedures, where enterprise-owned mobile devices are shared by clinicians rather than using clinicians’ personal devices. Virtually all respondents (99%) expect their deployment of shared-use mobile devices to increase over the next 12–24 months, with over half (51%) anticipating significant growth in use. In the US, 62% of facilities had fully implemented policies-procedures for managing shared-use mobile devices, with 58% in Canada, 53% in the UK, and 47% in Australia. Hospitals with 500–749 beds more frequently reported having fully implemented policies and procedures (71%) compared to those with less than 500 beds (57%), or with 750–1,000 beds (55%).
Survey respondents were aware of the importance of shared-use mobile access management, with 99% stating that improvement is needed in defining procedures for accessing applications and how data is controlled within their organizations. Further, respondents across nations stated that improvement is needed with respect to their facility or system efforts in auditing of device usage: 16% stated that their facilities have no consistent policy or process in place for assigning devices when a clinical shift begins; 46% use verbal or other informal processes for assigning devices; and 28% use a “first come, first served” method where staff members pickup any available device, with no systematic assignment process or documented checkout.
3.3Reported benefits of shared-use mobile devices
Almost all respondents across nations reported that care teams derive substantial benefits from using shared-use mobile devices in clinical workflows, with 94% reporting that they facilitate the delivery of high-quality patient care. Other widely perceived benefits included increased clinician satisfaction (94%), reduced clinician professional burnout (90%), reduced patient hospital length of stay (86%), enhanced care team coordination and communication (67%), improved access to clinical applications (54%), and acceleration of patient care delivery (51%) (see Figure 1).
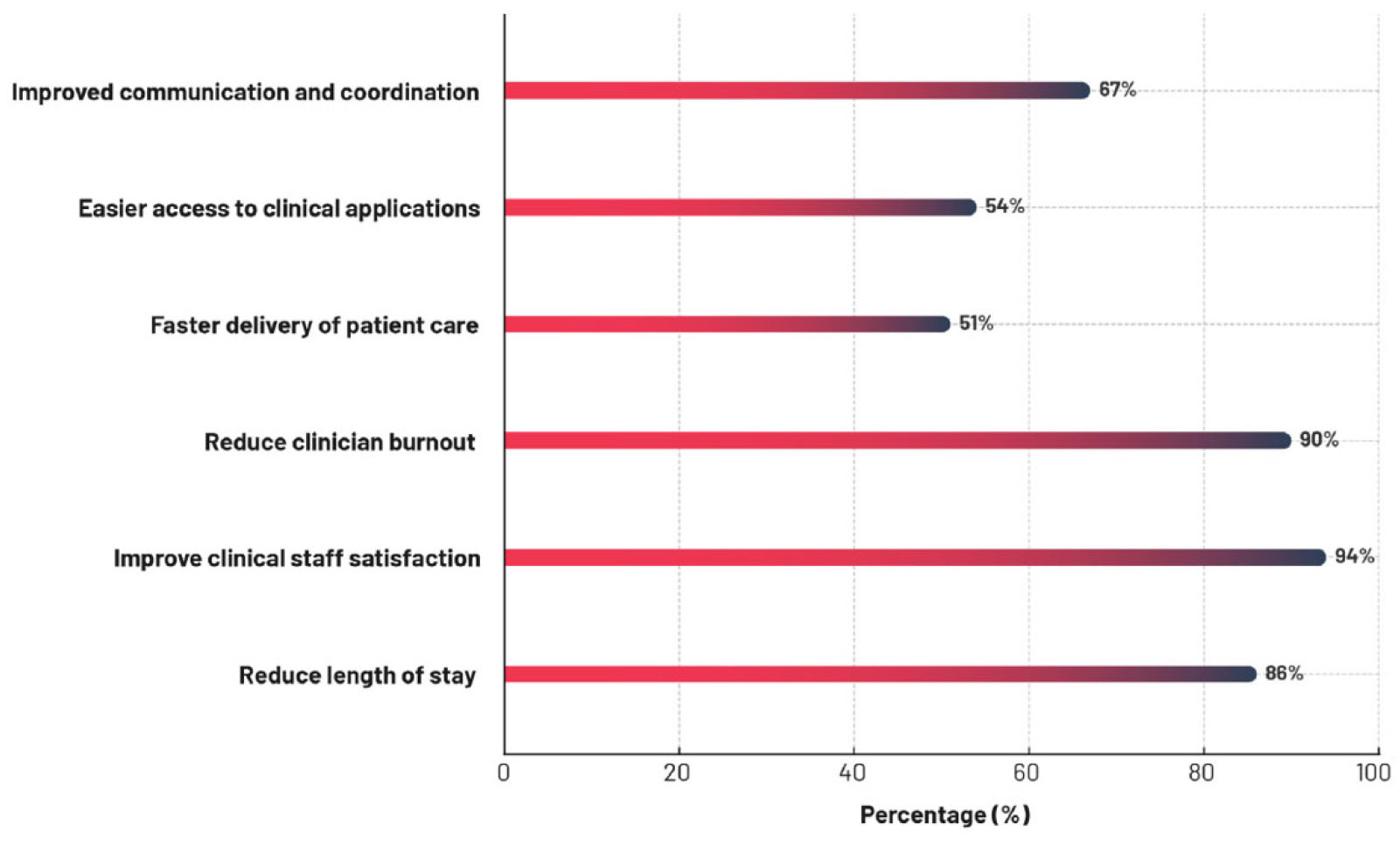
Figure 1.
All nation perceptions of clinical impact and value of shared-use mobile devices
The frequency with which respondents identified specific benefits of shared-use mobile devices was consistent across the four nations, with little inter-nation variation in completely or somewhat agreeing that a particular benefit is conveyed (see Table 2). The range of response frequencies were 90%–97% for improved clinical team communication; 84%–97% for facilitating high quality care; 87%–95% for expediting patient discharge; 87%–95% for increasing team productivity; 81%–89% for reducing patient length of stay; and 81%–89% for accelerating care delivery. A similar multinational consensus was reported for mobile devices yielding a favorable qualitative impact, including increased clinician work satisfaction (92%–95%) and reduced clinician work burden and professional burnout (87%–91%).
| Facilitates high quality care | Complete | 43% | 45% | 49% | 55% |
| Somewhat | 51% | 50% | 42% | 42% | |
| Improves clinical team communication | Complete | 52% | 55% | 46% | 52% |
| Somewhat | 45% | 42% | 44% | 41% | |
| Delivers more value than BYOD | Complete | 47% | 42% | 45% | 46% |
| Somewhat | 49% | 52% | 40% | 49% | |
| Helps reduce patient length of stay | Complete | 45% | 53% | 35% | 47% |
| Somewhat | 44% | 33% | 46% | 39% | |
| Decreases time to (accelerates) care delivery | Complete | 25% | 43% | 36% | 38% |
| Somewhat | 64% | 38% | 46% | 45% | |
| Expedites patient discharge process | Complete | 39% | 40% | 50% | 45% |
| Somewhat | 56% | 55% | 37% | 45% | |
| Reduces clinician work burden and burnout | Complete | 52% | 38% | 41% | 37% |
| Somewhat | 37% | 53% | 46% | 56% | |
| Increases clinician work satisfaction | Complete | 39% | 35% | 46% | 51% |
| Somewhat | 55% | 60% | 46% | 44% | |
| Increases productivity | Complete | 52% | 38% | 41% | 44% |
| Somewhat | 37% | 50% | 46% | 51% | |
3.4Greatest challenges in facilitating clinician access and ease of use of shared-use mobile devices
The most frequently identified challenge organizations face around shared-use mobile devices is maintaining the security of sensitive/protected data (44%). Risk increases with certain access workflows used by clinicians and operational IT challenges previously noted: 79% of respondents reported that individuals within their organization share credentials when accessing devices, and 74% indicated that staff frequently leave shared-use devices signed in after use, potentially exposing protected personal health information (PHI) or other sensitive data. These problems are reflected in almost half of respondents (49%) stating that they are not highly confident that patient data is fully protected on facility/enterprise shared-use mobile devices.
Sixty-two percent of respondents reported that care staff experience issues accessing shared-use mobile devices somewhat or very often despite facility efforts to make device deployment frictionless and user-friendly. Seventy-five percent of respondents stated that clinicians frequently have to contact the help desk to remediate being locked out of mobile devices or applications, increasing service demand on the information technology management team. Helpdesk tickets were estimated to cost an average of $70 per opened ticket, and respondents indicated that improved shared-use mobile management capabilities could help minimize avoidable calls to the help desk by streamlining authentication and access processes, potentially rendering considerable cost savings.
A large majority of survey respondents (87%) reported that clinicians experience access issues and frustrations when devices are not available for immediate use, which in turn hampers care team communications and causes delays in patient care delivery. Usability issues such as devices being broken, not charged, or lacking the right applications and tools were reported by 86% of respondents. Other frequently reported workflow challenges for clinicians included inconsistent configuration of applications (39%), and time-consuming device authentication processes (36%). Table 3 identifies key facility management challenges in deploying shared-use mobile devices. A moderately high degree of consistency in responses across the four nations is evident.
| Clinicians share login credentials | Complete | 39% | 35% | 40% | 30% |
| Somewhat | 44% | 48% | 37% | 48% | |
| Devices are frequently left signed in by staff | Complete | 31% | 32% | 35% | 30% |
| Somewhat | 47% | 43% | 38% | 41% | |
| Personal devices used as a workaround when shared-use mobile devices are unavailable | Complete | 39% | 38% | 33% | 40% |
| Somewhat | 44% | 43% | 45% | 41% | |
| Clinicians reluctant to use mobile devices due to workflow frustrations | Complete | 25% | 38% | 17% | 28% |
| Somewhat | 41% | 32% | 27% | 38% | |
| Clinicians frequently contact the help desk to remediate lock outs of devices or applications | Complete | 35% | 43% | 42% | 25% |
| Somewhat | 45% | 33% | 32% | 49% | |
Table 4 conveys organizational challenges in deploying shared-use mobile devices by facility size as reflected by total bed count. Larger hospitals and particularly those with 500–749 beds tended to report clinician challenges more frequently than smaller facilities.
| Clinicians share login credentials | Complete | 21% | 26% | 34% | 41% | 51% |
| Somewhat | 44% | 42% | 51% | 42% | 39% | |
| Devices are frequently left signed in by staff | Complete | 18% | 28% | 40% | 28% | 39% |
| Somewhat | 38% | 37% | 42% | 46% | 45% | |
| Personal devices used as workaround when shared-use mobile devices are unavailable | Complete | 26% | 38% | 47% | 35% | 34% |
| Somewhat | 38% | 40% | 41% | 47% | 48% | |
| Clinicians reluctant to use mobile devices due to workflow frustrations | Complete | 13% | 22% | 29% | 22% | 35% |
| Somewhat | 26% | 32% | 33% | 34% | 30% | |
| Clinicians frequently contact help desk to remediate devices or application lock outs | Complete | 36% | 34% | 35% | 34% | 0% |
| Somewhat | 21% | 43% | 48% | 34% | 0% | |
3.5Frequency of clinicians reporting problems in utilizing shared-use mobile devices
Respondents were asked to identify the frequency that clinical users encounter problems acquiring, accessing, or using shared-use mobile devices. Across nations issues are encountered frequently by clinicians when using a shared-use mobile device. Clinicians working in the UK and the US report somewhat lower but still substantial rates of all three problems (see Table 5).
| Availability (mobile devices are not available, are missing, or there is inadequate inventory) | Very often | 27% | 48% | 20% | 25% |
| Somewhat often | 40% | 25% | 30% | 25% | |
| Accessibility (getting locked out of a mobile device) | Very often | 28% | 42% | 22% | 26% |
| Somewhat often | 44% | 37% | 30% | 33% | |
| Usability (mobile devices are broken, not charged, and lack the right applications/tools) | Very often | 31% | 33% | 34% | 31% |
| Somewhat often | 41% | 37% | 26% | 26% | |
Table 6 identifies problems reported by clinicians about shared-use mobile devices by facility size. Clinicians working at larger hospitals reported problems more frequently than those working at smaller facilities, and the frequency of reporting problems appears to have a direct linear relationship with facility size.
| Availability (mobile devices are not available, are missing, or there is inadequate inventory) | Very often | 15% | 18% | 27% | 33% | 39% |
| Somewhat often | 18% | 30% | 33% | 22% | 39% | |
| Accessibility (getting locked out of a mobile device) | Very often | 18% | 22% | 30% | 19% | 44% |
| Somewhat often | 18% | 25% | 39% | 51% | 34% | |
| Usability (mobile devices are broken, not charged, and lack the right applications/tools | Very often | 13% | 16% | 32% | 47% | 48% |
| Somewhat often | 18% | 31% | 34% | 27% | 36% | |
3.6Greatest challenges in facility management of shared-use mobile devices
Figure 2 presents shared-use mobile device fleet management challenges reported for the IT management team. These included a lack of visibility into mobile device usage (40%), lack of a centralized system for managing devices (39%), time-consuming device setup processes (35%), and lack of a reliable way to track mobile devices (35%). Further, respondents cited challenges relating to a lack of visibility into which users were assigned a particular device (48%); when specific devices were last assigned (53%); and what applications are being accessed on mobile devices (55%). There was marginal variability in the reporting of these challenges across nations.
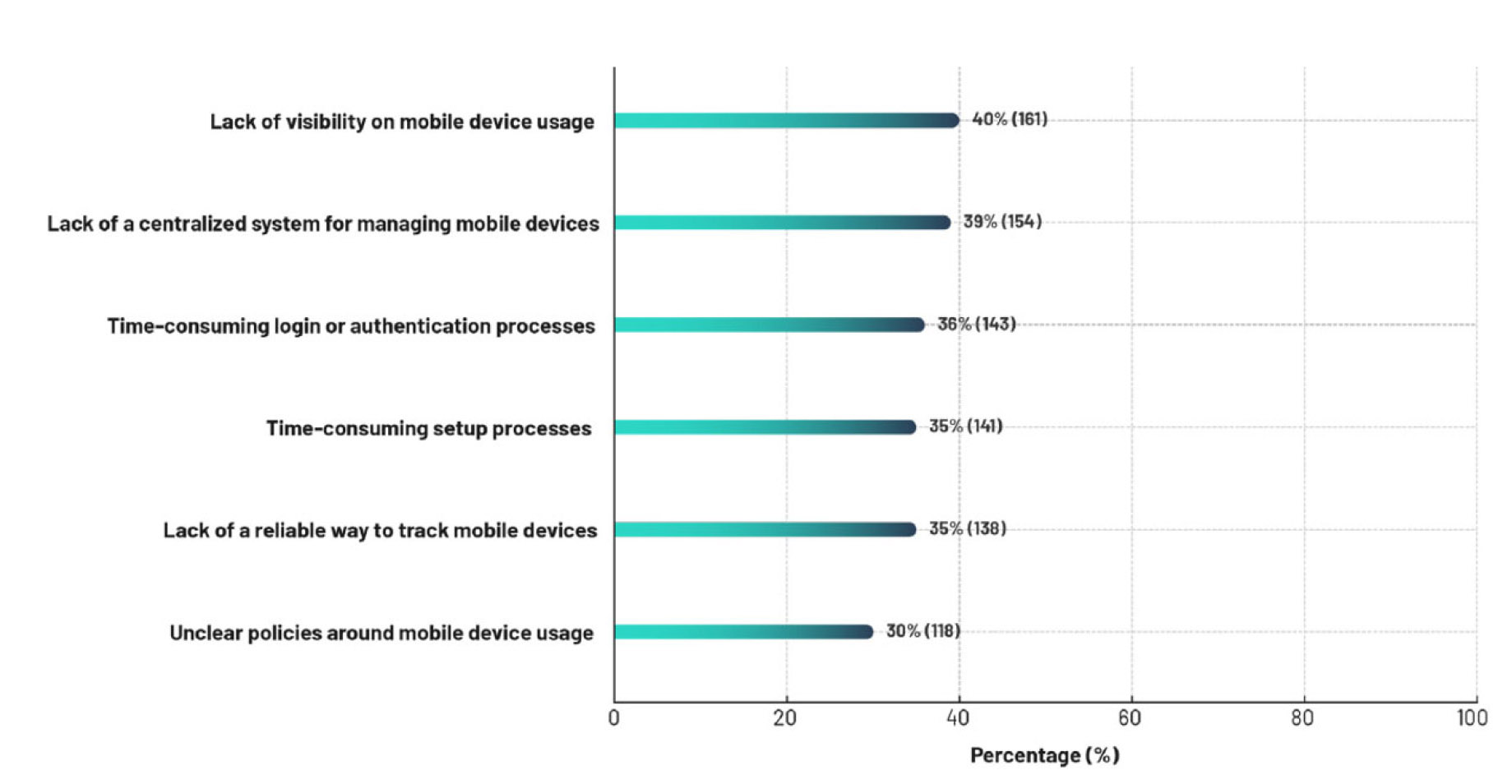
Figure 2.
Shared-use mobile device management challenges for the information technology department
When shared-use devices are not available or difficult to access, 81% of respondents stated that personal devices are used instead. This workaround undermines an organization’s investment in shared-use devices and creates the risk of new opportunities for attack vectors to threaten information security and privacy. The time required to assign a shared-use mobile device to a clinician varied by nation: 50% of respondents in the UK stated that device assignment requires five minutes or less, whereas in Australia 39% so indicated, with the US and Canada reporting longer times in excess of 10 minutes, with only 26% so stating in Australia and 25% in the UK.
Frequently reported access frustrations included outdated authentication methods, with 26% still relying predominantly on usernames and passwords to access mobile applications. Productivity losses often begin before a shift starts due to device assignment challenges. Respondents indicated that a mean of 13 minutes were required to assign a shared-use mobile device to a member of the care team. Reasons for this included limited availability of mobile devices (40%), unnecessarily time-consuming handover processes between shifts (39%), use of manual or legacy processes for device allocation (35%), inconsistent policies/procedures for device assignment (35%), and uncharged device battery (35%).
Table 7 details facility challenges in deploying shared-use mobile devices by nation. Substantial percentages of facilities across all four nations are experiencing a variety of mobile device fleet management issues, with little inter-nation variability in specific problems identified.
| Data security concerns | 51% | 38% | 47% | 39% |
| Lack of visibility into mobile device usage | 48% | 40% | 38% | 39% |
| Devices not configured with needed applications | 41% | 40% | 44% | 33% |
| Lack of centralized system for managing mobile devices | 49% | 42% | 39% | 31% |
| Time-consuming login or authentication processes | 36% | 32% | 36% | 37% |
| Time-consuming setup processes | 32% | 30% | 38% | 36% |
| Lack of a reliable way to track mobile devices | 39% | 40% | 40% | 25% |
| Have no challenges in using shared-use mobile devices | 0% | 0% | 4% | 5% |
Table 8 stratifies reported facility mobile device management challenges by facility size. No clear trends by hospital size are apparent.
| Data security concerns | 44% | 56% | 40% | 40% | 36% |
| Lack of visibility into mobile device usage | 38% | 36% | 42% | 45% | 40% |
| Devices not configured with needed applications | 26% | 38% | 37% | 44% | 45% |
| Lack of centralized system for managing mobile devices | 31% | 33% | 42% | 42% | 41% |
| Time-consuming login or authentication processes | 31% | 30% | 38% | 44% | 35% |
| Time-consuming setup processes | 18% | 37% | 34% | 39% | 40% |
| Lack of a reliable way to track mobile devices | 28% | 33% | 36% | 35% | 38% |
| Have no challenges in using shared-use mobile devices | 10% | 3% | 0% | 1% | 5% |
3.7Current state of shared-use mobile device tracking and utilization visibility
Table 9 shows how mobile devices are tracked by respondent facilities, demonstrating that multiple methods, including antiquated ones, are commonly employed by healthcare delivery organizations. Inefficient and sub-optimal tracking occurs through continued reliance on manual sign-out paper logs and manual digital logs (e.g., Microsoft Excel spreadsheets) by a substantial percentage of HDOs.
| Real-time location system or geolocation technology | 68% | 52% | 54% | 56% |
| Mobile device management platform | 60% | 47% | 48% | 51% |
| Staff login credentials (e.g., badge tap) | 36% | 33% | 52% | 46% |
| Smart charging/docking station with built-in tracking | 44% | 42% | 49% | 40% |
| Barcode scanning or radio frequency identification tracking | 52% | 42% | 42% | 35% |
| Manual sign-out sheet or paper log | 40% | 37% | 43% | 27% |
| Manual digital log (e.g., Microsoft Excel) | 27% | 23% | 36% | 34% |
| Facility does not track location of devices or other | 0% | 0% | 2% | 0% |
Table 10 conveys the reported level of visibility that HDOs have into key utilization metrics critical to the effective management of a fleet of shared-use mobile devices. Little international variation in reporting is evident.
| Who has accessed or been assigned a mobile device | 41% | 48% | 50% | 49% |
| When the mobile device was last assigned | 56% | 57% | 51% | 50% |
| What applications are being accessed | 53% | 52% | 64% | 49% |
| How often applications are being accessed | 63% | 53% | 54% | 56% |
| Departments using mobile devices and to what extent | 56% | 50% | 52% | 44% |
3.8Impact of shared-use mobile device loss on clinical care operations and delivery
The substantial frequency of shared-use mobile device loss is another costly challenge respondents reported, with a mean of 23% of the facility fleet of devices lost annually. The high cost of loss derives not only from purchasing replacements of lost devices, but from lost productivity as well. In addition to direct financial costs, missing mobile devices cause an average clinician downtime of three hours per device as access to key workflows and applications is impeded. Locating a missing mobile device may require up to a full shift (12 hours) to locate. Figure 3 details other negative consequences of missing, misplaced or unavailable shared-use mobile devices.
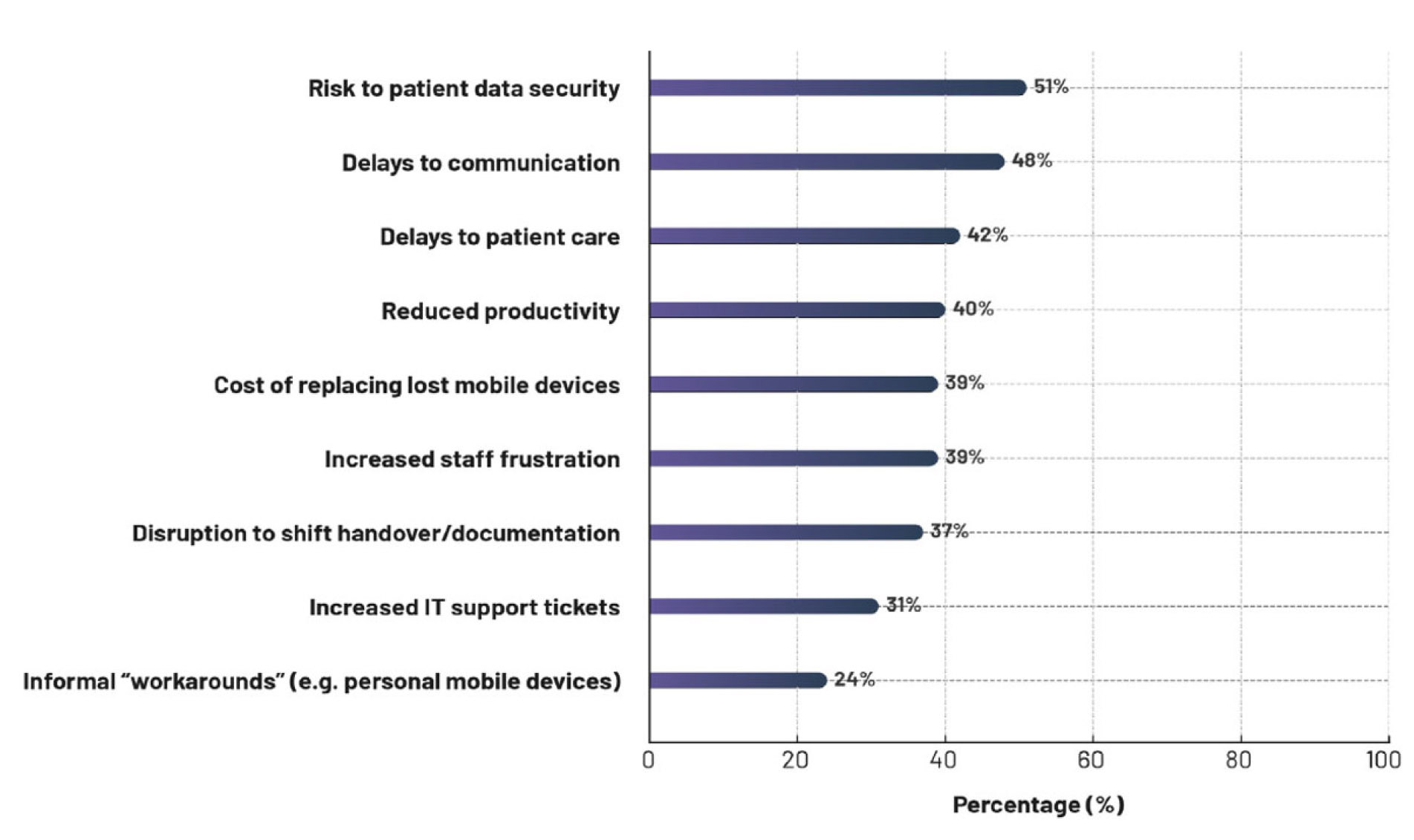
Figure 3.
Impact of missing, misplaced or unavailable shared-use mobile devices on care teams
3.9Impact of missing, misplaced or unavailable shared-use mobile devices on patient care delivery
Table 11 details the negative effects missing, misplaced and unavailable shared-use mobile devices have on the delivery of patient care by clinicians.
| Risk to patient data security | 55% | 46% | 48% | 55% |
| Communication delays | 58% | 33% | 48% | 49% |
| Patient care delays | 39% | 50% | 40% | 44% |
| Reduced productivity | 39% | 29% | 48% | 38% |
| High avoidable device replacement cost | 42% | 38% | 40% | 38% |
| Clinician frustration | 42% | 38% | 48% | 29% |
| Disruption of shift transitions | 52% | 33% | 35% | 31% |
| Increased IT support ticket requests | 35% | 25% | 38% | 25% |
| Increased use of workarounds/personal device use | 23% | 21% | 27% | 24% |
| No impact, other impact or do not know impact | 0% | 0% | 2% | 2% |
Table 12 stratifies reporting on the impact of missing or unavailable shared-use devices by facility size. Smaller facilities of 100–249 and 250–499 beds size tended to more frequently report risk to patient data security and high avoidable device replacement cost, while those with 1,000+ beds reported patient care delays and increased IT support ticket requests.
| Risk to patient data security | 57% | 66% | 46% | 41% | 43% |
| Communication delays | 39% | 46% | 49% | 59% | 47% |
| Patient care delays | 52% | 39% | 41% | 33% | 50% |
| Reduced productivity | 43% | 41% | 41% | 37% | 37% |
| High avoidable device replacement cost | 61% | 46% | 32% | 26% | 33% |
| Clinician frustration | 43% | 37% | 38% | 41% | 37% |
| Disruption of shift transitions | 22% | 34% | 43% | 44% | 37% |
| Increased IT support ticket requests | 13% | 32% | 32% | 22% | 50% |
| Increased use of workarounds/personal devices | 17% | 17% | 35% | 15% | 33% |
| No impact, other impact or do not know impact | 0% | 2% | 0% | 0% | 7% |
3.10Time spent locating missing or misplaced shared-use mobile devices
Substantial IT management time is spent locating missing shared-use mobile devices. High rates of mobile device loss can be attributed in part to outdated tracking methods, with a third of respondents stating their facility still relies on manual sign-out sheets (36%) or Microsoft Excel (32%) to track the locations of devices (see Table 6). Across nations, locating a missing device can take significant time: 33% of Australian respondents, 67% of Canadian respondents, 27% of UK respondents and 34% of US respondents indicated that it may take upwards of six hours to locate a device (see Table 13).
| Less than 1 hour | 17% | 7% | 26% | 33% |
| 1 to less than 6 hours | 51% | 27% | 43% | 33% |
| 6-12 hours | 20% | 48% | 19% | 25% |
| Several days | 7% | 12% | 6% | 9% |
| One week | 3% | 5% | 2% | 0% |
| Several weeks | 3% | 2% | 0% | 0% |
3.11Financial benefit of shared-use mobile devices
HDOs reported saving a mean of $1.1 million annually by using shared-use devices over individually-allocated ones. The survey item regarding cost only asked respondents to estimate how much their care facility saves annually by deploying shared-use mobile devices rather than dedicated user mobile devices, without seeking details on how these financial estimates were completed. Lacking clarity and consistency of determination, this $1.1 million in annual savings should be regarded as a crude estimate.
Almost universally decision makers expect shared-use mobile device deployment to grow over the next two years. Yet, if not managed properly, transition to shared devices involves challenges: policy gaps, access inefficiencies and security concerns. Sixty-two percent of respondents stated care staff often experience issues accessing shared-use mobile devices, and 23% of devices are lost annually. Many struggle to manage shared-use mobile devices, and manual processes to assign/track them are common.
For IT teams, shared-use mobile devices reduce manual workload, which frees them to focus on other high priority projects that deliver additional value to the organization. The leading benefits of shared-use mobile devices for IT were consistent with little variability across nations, and included improved asset management in locating lost devices (66%); increased alignment with regulations and compliance requirements (65%); enhanced data security (60%); and greater visibility into mobile device usage and accountability (59%). Compared to 1:1 dedicated-user or BYOD devices, shared-use devices provided cost savings, with 92% of survey respondents stating that shared-use devices deliver greater return on investment. Respondents from organizations with fully implemented shared-use device policies and operating procedures reported a 63% greater return on investment than those lacking them, with a reported mean annual savings of $1.4 million versus $860,000, respectively (see Figure 4).
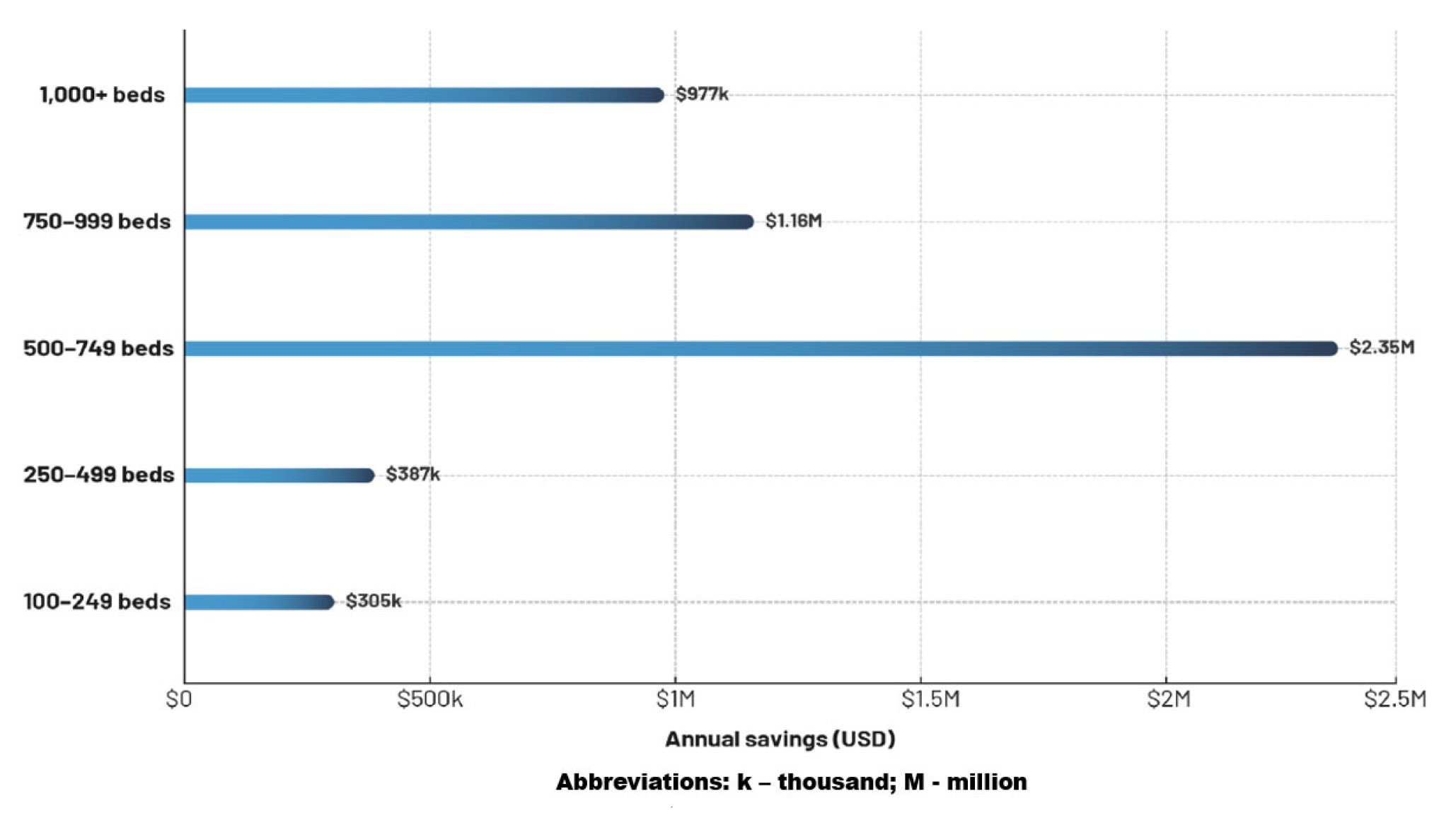
Figure 4.
Annual savings of shared-use mobile devices by facility number of beds
4.Discussion
4.1Summary of key findings
The findings evidence a gap between HDO aspirations for introducing and supporting mobile initiatives—with 92% agreeing that mobile devices are becoming essential tools within the care delivery IT ecosystem—and the realities of current capabilities, where only 56% across nations have fully implemented systematic shared use policies and procedures. No consistent pattern emerged differentiating nations in this regard, or according to number of facility beds, or perceived benefits of shared-use mobile devices in care delivery. The most highly ranked benefits across nations were improved clinician satisfaction, a reduction in clinician burnout or fatigue and, strikingly, reduced inpatient length of stay. Almost all respondents expect their deployment of shared-used mobile devices to increase over the near term.
Challenges in facilitating clinician access and ease of use of shared-use mobile devices were endemic, and included concerns around maintaining information security and protection of sensitive protected data, with reported issues such as clinicians sharing access credentials, leaving devices logged in after individual use, and ensuring access is rapid and frictionless. Frequency of clinicians needing to contact the help desk when locked out of a mobile device was higher than desired, this being an associated avoidable cost. These problems, plus usability impediments such as devices being broken, not charged, or lacking needed clinical applications and inconsistent application configuration, were perceived as impeding effective clinical staff communications, workflow and productivity/patient throughput. Little variation was observed between nations, with the exception of slightly lower issue reporting in the UK and US.
International consistency was also evident in responses about IT team or department management of shared-use mobile devices. Respondents often reported lack of visibility into and ability to track mobile device usage via a centralized mobile device management system, along with time-consuming authentication and setup processes. When access is difficult, clinicians employ unsafe workarounds to achieve access, such as using personal mobile devices. A very limited number of respondents stated their facility faces no challenges in deploying shared-use mobile devices; none in Australia and Canada and only 4% of respondents in the UK and 5% in the US. Substantial minorities across nations reported still relying on manual sign-out/paper or manual digital monitoring of device sign-out. Respondents reported insufficient visibility into critical mobile device use metrics, including who has accessed or been assigned a particular device, when assigned, which applications are being accessed and with what frequency, and by which hospital department.
Besides a high mean rate of annual mobile device loss (23% across nations), the impact of missing and misplaced/unavailable mobile devices on care teams was reportedly serious in nature, including not only increased risk of information security breach, but also delays in clinical team communications and patient care delivery, as well as reduced productivity, disruption of shift change or transition, and increased staff frustration. The time required to located a missing device was typically 1–12 hours, with Canada reporting longer durations. Many of these findings are consistent with those in other reports.[8, 10]
Nonetheless, hospitals reported meaningful savings by deploying shared-use mobile devices of $1.1 million per annum on average, with 92% indicating a meaningful return on investment, and reduced manual workload for IT teams. Other reported benefits over a BYOD approach included improved asset management, better alignment with regulations and compliance imperatives, and enhanced data security (with little variation between nations).
4.2Implications of study findings
It is clear from the findings reported that an informal or inconsistent approach to shared-use device assignment, monitoring and management creates workflow issues and a lack of accountability, while also increasing security and breach of privacy risks for HDOs. Lack of unified or integrated mobile device management tools prevents hospitals from achieving visibility into device use metrics and enforcing consistent access controls and data usage policies facility- or enterprise-wide. While HDOs appreciate the value of shared-use mobile devices, many are not satisfied with their current capabilities to do so. Respondents commonly reported inferior, incomplete or non-existent capabilities for managing a mobile device fleet that ensures cybersecurity, clinician ease of use, reduced IT staff burden, and which minimizes costly losses of devices.
Yet identity-driven solutions exist that can help HDOs optimize mobile device clinical productivity by easing mobile device access/authentication and management workflows while increasing visibility into mobile device usage, mitigating data security risks and reducing the support burden on the IT department.[8] Across nations, HDOs perceive the lack of effective shared-use mobile device management capabilities as a significant source of unnecessary costs, lost clinician and IT team productivity, and inefficient human resource management. An enterprise shared-use device access management capabilities set or solution can assist HDOs in their efforts to reduce adoption barriers and maximize the impact of facility or system investment in mobile device technology. Clinician use of shared mobile devices can be simplified and enhanced by deploying existing technology platforms that enable a clinician to check out a device by just tapping their identity badge for access/authentication during their entire shift.[8] An identity-driven approach also facilitates ease of communication between clinicians, and ensures they can contact the right person rapidly and easily, important in care delivery and particularly in emergent situations. By investing in purpose-built technologies and implementing policies and processes that address the unique needs of shared-use mobile device management, healthcare organizations can maximize the clinical and operational value of shared-use mobile devices while mitigating risks associated with device loss and data breaches.[8]
4.3An identity-driven solution using a centralized mobile device management platform
One illustration of technological advancement in solutions to help HDOs meet the challenges of mobile device management is the Mobile Access Management (MAM) solution from Imprivata, which conveys a foundation for secure and efficient access to shared mobile devices used in clinical environments. The platform enables controlled assignment and rapid authentication workflows. Through the use of Launchpad workstations, badge readers, and Smart Hub docks, MAM allows clinicians to check out a mobile device with a simple proximity badge tap. The device is immediately and automatically associated with that user for the duration of the session. A Locker application enforces session separation, ensuring that no residual data, application state, or device unlock method persists between uses. This approach reduces common risks in shared-use environments, such as lingering credentials, persistent application sessions, or unlocked devices left active between handoffs. By standardizing the check-out and return process, MAM also supports consistent availability of devices at the start of each shift, helping to reduce delays and workflow disruptions affecting hospital mobility programs.
MAM integrates with Imprivata Enterprise Access Management, enhancing mobile workflows by extending the same authentication and single sign-on capabilities clinicians rely on at shared workstations to shared mobile devices. When clinicians check out a device, MAM leverages enterprise access management (EAM) to provide fast, password-less access to hospital applications, including secure communication tools and mobile electronic health record (EHR) interfaces. This reduces repetitive manual logins and minimizes lockouts, which are a major contributor to help-desk service demand and clinician frustration. Because the device is depersonalized at check-in, access tokens and application sessions are not carried forward to the next user, thereby improving security while maintaining efficiency. In addition, MAM generates detailed audit logs of device assignment, session duration, charging status, and missing device events, providing IT teams with needed visibility into how and when devices are being used. These data help hospitals identify patterns of mobile device loss or underutilization, inform asset management, and improve accountability in environments where device loss rates can be operationally and financially problematic. Together, MAM and EAM support a secure, rapid, and predictable mobile access model tailored to the realities of shared-use clinical mobility and the needs of HDOs.
4.4A framework for HDOs transitioning from manual to automated mobile device management
HDOs transitioning from manual mobile device processes to automated, access-managed shared-device programs can benefit from adopting a structured implementation framework that emphasizes workflow validation, phased deployment, and alignment across clinical, IT, and informatics teams. Imprivata’s Mobile Access Management (MAM) platform, for example, is typically introduced through a staged migration in which hospitals begin by defining clinical use cases, mapping staffing levels to mobile device inventory, and identifying workflow bottlenecks such as lengthy device handoffs, inconsistent authentication steps, or unpredictable device availability. Documentation from the platform identifies these early phases as critical for operational readiness, recommending pre-deployment assessments of charging infrastructure, network coverage, and departmental device distribution patterns.
The programmatic approaches applied at institutions such as Boston Children’s Hospital demonstrate the value of centralized data collection, early identification of clinical champions, and regular coordination across technology support, enterprise systems, and clinical groups to ensure that mobile workflows remain consistent with established clinical communication and application pathways. Change management and training strategies are central to a successful and frictionless transition from manual to automated device management. Effective adoption requires a combination of early awareness generation efforts, hands-on training, and scalable instructional models such as “train-the-trainer” approaches. This is supported through predictable, repeatable device check-in/check-out workflows, and integration with EAM for badge-based authentication, thereby reducing user complexity and allowing training to focus on clinical efficiency rather than device mechanics.
Implementation teams commonly incorporate super users, in-person training sessions, tip sheets, short instructional videos, and just-in-time micro-training to orient and support shift-based clinical staff. Post-deployment, MAM analytics give IT and operational leaders visibility into device assignment patterns, loss trends, and department-level utilization; these data inform continuous improvement cycles and help validate whether training or workflow changes are required. This structured combination of technical instrumentation, cross-departmental coordination, and iterative training ensures that hospitals replacing manual processes with automated shared-device management can achieve widespread adoption of mobile devices by ensuring consistent device availability, reduced shrinkage, and support of more reliable mobile workflows at the point of care.
4.5Study limitations
Several methodological limitations and constraints need to inform the interpretation and generalizability of the reported findings. As a web-based survey, the data reported data may be subject to biases, including sampling frame bias and non-response bias. When surveys are sent to a representative sample of individuals, sampling frame bias could exist if the respondents selected for participation are not truly representative of the intended or target group of respondents. In addition, individuals who did not respond and participate in the survey may be substantially and systematically different in terms of responses from those who did participate, introducing potential non-response bias. The study’s use exclusively of self-reported data may also limit the interpretation of the findings presented. The quality of information derived from a self-reported survey depends on the integrity of confidential responses received from subjects. While the study methods included response validity and consistency checks within the survey process, not all subjects may have provided accurate and truthful responses. Furthermore, because a web-based data collection method was used, it is possible that non-web based responses by a mailed survey or a telephone survey might have yielded systematically different findings than those presented. Given the expected high growth in shared-use device deployment in coming years, future research should engage longitudinal follow-up studies to track changes in device management practices and outcomes over time.
5.Conclusions
HDOs clearly understand that shared-use mobile devices offer much value in improved clinician workflow and enhanced use of point-of-care applications, team communication and coordination, and productivity if effectively and efficiently managed. Implementing rapid and easy to use yet secure user authentication methods on shared-use devices remains a significant challenge for many hospitals and healthcare systems. Capability gaps and challenges reported by HDOs were largely consistent and shared across the four nations surveyed. Greater visibility into and accurate real-time reporting of mobile device usage metrics are widely perceived as unmet imperatives. HDOs need mobile device management solutions that can overcome the barriers and impediments reported, reduce clinician friction during access and use, and facilitate mobile device workflows and productivity through expedited mobile device authentication and clinical application/information access.[8, 10] Need exists to deploy appropriate technology solutions that enable and support implementation of such systematic policies and workflows.
Existing shared-use mobile device management solutions can help HDOs reduce costs, improve access ease and security, and enhance clinician user experience and satisfaction, while reducing IT department administrative burden.[8, 10] With such capabilities in hand, HDOs may better integrate this powerful addition to the healthcare information ecosystem to bring clinical applications and patient data to the bedside, which can result in better and more patient-centric care. Robust, effective and efficient shared-use mobile device management can reduce clinician information technology fatigue and burnout by expediting workflows and increasing care efficiency, while reducing IT department burden and costs. With investment in and deployment of appropriate mobile device management capabilities, clinical mobility can emerge as a new operating standard in global medicine.
Authors contributions
DB and RP designed the study methodology; DB, RP, SPK and GAG analyzed and interpreted the data; GAG wrote the initial and all subsequent drafts of the manuscript; DB, RP and SPK edited subsequent drafts of the manuscript; GAG and RP organized the data and validated the data analyses; GAG, DB and RP co-authored the results interpretation and discussion sections.
Funding
No funding supported this work.
Conflicts of Interest Disclosure
All authors are either advisors to or employees of Imprivata.
Informed consent
Survey respondents provided their consent for their interview data to be used in a fully de-identified manner within aggregate analyses.
Ethical statement
All data were collected observing strict data confidentiality, privacy and ethical research standards. All respondents opted in to survey participation and accepted the survey terms that declared their individual data would be analyzed and presented in aggregate form and a fully de-identified manner. No personally identifiable information from individuals was collected. As a result, Ethical Board review was waived.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
Study data may be made available upon reasonable request.
Data sharing statement
No additional data are available.
Acknowledgements
None.
References
- Lee M, Bin Mahmood A, Lee E. Smartphone and mobile app use among physicians in clinical practice: Scoping review. J Med Internet Res Mhlth Uhlth. 2023;11:e44765. doi:10.2196/44765
- Juniper Research. Smart hospitals to deploy over 7 million Internet of medical things. January 2022. https://www.juniperresearch.com/press/smart-hospitals-to-deploy-over-7mn-iomt/
- Nerminathan A, Harrison A, Phelps M. Doctors’ use of mobile devices in the clinical setting: A mixed methods study. Intern Med J. 2017;47(3):291-298. doi:10.1111/imj.13349
- Alsabah M, Naser M, Albahri A. A comprehensive review on key technologies toward smart healthcare systems based IoT: technical aspects, challenges and future directions. Artif Intell Rev. 2025;58:343. doi:10.1007/s10462-025-11342-3
- Zhu H, Wu C, Koo C. Smart healthcare in the era of internet-of-things. IEEE Consum Electron Mag. 2019;8(5):26-30. doi:10.1109/MCE.2019.2923929
- Sim I. Mobile devices and health. N Engl J Med. 2019;381:956-968. doi:10.1056/NEJMra1806949
- JAMF (Just Apple’s Management Framework). Survey: The impact of mobile devices on hospital patient satisfaction. 2018. https://www.jamf.com/resources/e-books/2018-survey-the-impact-of-mobile-devices-on-hospital-patient-satisfaction/
- Gellert G, Stanton G, Paulemon M. Challenges and opportunities in achieving secure hospital mobility management: An illustrative use case. J Hosp Admin. 2024;13(2):1-9. doi:10.5430/jha.v13n2p1
- Jennings A. Hidden costs of missing medical equipment. Chief Healthcare Executive. Hidden costs of missing medical equipment. Viewpoint. August 28, 2023. https://www.chiefhealthcareexecutive.com/view/hidden-costs-of-missing-medical-equipment-viewpoint
- Gellert G, Gellert G, Pickering R. The love-hate state of mobile device management in healthcare: An international survey. Informatics Med Unlock. 2025;52:101603. doi:10.1016/j.imu.2024.101603
- Imprivata. Unlocking the Cost of Chaos: The State of Enterprise Mobility in Life-and Mission-Critical Industries. March 2024. https://www.imprivata.com/company/press/unlocking-cost-chaos-state-enterprise-mobility-life-and-mission-critical-industries
- Zakerabasali S, Ayyoubzadeh S, Baniasadi T. Mobile health technology and healthcare providers: Systemic barriers to adoption. Healthcr Informn Res. 2021;27(4):267-278. doi:10.4258/hir.2021.27.4.267
- Wosny M, Strasser L, Hastings J. Experience of health care professionals using digital tools in the hospital: Qualitative systematic review. JMIR Hum Factors. 2023;10:e50357. doi:10.2196/50357
- Borges do Nascimento I, Abdulazeem H, Vasanthan L. Barriers and facilitators to utilizing digital health technologies by healthcare professionals. NPJ Digit Med. 2023;6(1):161. doi:10.1038/s41746-023-00899-4
 This work is licensed under a
This work is licensed under a 