1.Introduction
Clinical environments are often complex and fast-paced, demanding that individuals work cohesively in teams, follow standard operating procedures, share information within and across disciplines, and make sound decisions using accurate information. Meeting these demands requires good communication and an understanding of human factors principles, emphasizing that while human error is unavoidable, patient harm is not.[1] Clinical Team Training (CTT), a multidisciplinary program based on aviation’s Crew Resource Management (CRM), was established to improve patient safety at Veterans Health Administration medical facilities, where various teams deliver care within a larger system. CTT seeks to influence the culture of the Veterans Health Administration (VHA) healthcare system, guiding it towards adopting a high reliability mindset. The larger system can be enhanced to manage and trap human error before small errors become bigger problems.
Joint Commission statistics (2004-2013) indicate that approximately 70 percent of the time, communication failures are cited as a significant root cause in reported sentinel events. CTT has demonstrated effectiveness at improving communication and teamwork in the clinical environment. A Veterans Affairs (VA) study found a significant decrease in the annual surgical mortality rate in groups trained in CTT methods as opposed to untrained groups. The 74 facilities in the training program experienced an 18 percent reduction in yearly mortality compared with a 7 percent decrease among the 34 facilities that had not yet undergone training. Two other studies showed further positive results from using CTT methods, such as a substantial decrease in the rate of adverse events and the severity of those events in the operating room. CTT methods were also implemented to improve communication and teamwork in 11 nursing units at nine VA facilities during another training program piloted in 2010. The implementation included a six-hour learning session and two-hour clinical simulations using high-fidelity patient simulators.[1, 2, 3]
Across several studies related to team training, there were demonstrated increases in patient safety as evident by reduced adverse events, such as errors in the operating room due to lack of preprocedural verifications. Along with enhanced teamwork behaviors, these studies showed that team training positively impacted clinical processes and patient outcomes. The significant findings included the importance of leadership involvement and interactions with project champions that positively impacted improved teamwork, ultimately resulting in overall quality improvements. Additionally findings showed evidence that CTT improved intragroup positive relationships, improved communication, and promoted standardization of processes resulting in fewer errors and improved patient outcomes.[3, 4]
There is also discussion in the literature suggesting that leadership responsible for organizational change should consider designing and implementing team training in annual planning events.[4] A study in 2016 demonstrated that the use of team training during annual planning optimized effectiveness of certain critical areas within healthcare operations settings. Investigators discovered an increase in employee engagement that indicated the same number of staff were able to achieve positive outcomes for patients due to improved working relationships and communication. Additionally, there were signs of significant improvement in organizational learning, supervisor and manager expectations, improved teamwork, a reduction of nosocomial infections, reduced falls, and a decrease in patient safety adverse outcomes. Finally, the study determined that leadership support was critical for this success.[5]
A notable finding relating to evidence on HRO implementation effects in an acute care study revealed that organizations experienced significant reductions in serious safety events (SSEs) (range from 55% to 100%). These improvements were maintained over a nine-year period. Staff who provided feedback during interviews agreed that leadership rounding is associated with an improved patient safety culture, higher employee engagement, and lower burnout.[6]
In March of 2021, the National Center for Patient Safety (NCPS) leadership aligned with the enterprise-wide implementation of the CTT program. CTT training can be compared to several quality improvement initiatives within the current literature. CRM, Life Flight and the TeamSTEPPS® Program are examples.[7] These training goals are very similar: increasing patient safety through improving the physical structure of the work environment, communication, standardizing processes, and open and honest dialogue relating to the human potential for mistakes to reduce harm. Organizations have the opportunity to improve human factors that impact the delivery of care and training, resulting in fewer errors through the use of a formalized safety training program. Nearly all participants reported positive outcomes post-intervention and training of CRM, including improved safety numbers.[1]
The current study aims to determine the facilitating factors and barriers to conducting large-scale CRM-based training in a national health care system (VHA). While there are some studies on this topic, none review training in a federal system or provide data on changes within the system.[1, 3, 4, 5, 7]
2.Methods
2.1The Veterans Health Administration
The VHA is America’s largest integrated health care system, including approximately 171 medical centers and 1,113 outpatient clinics serving 9 million enrolled Veterans each year.[8]
2.2The Clinical Team Training Program in VHA
The CTT program allows clinicians to improve patient safety by facilitating clear and timely communication through collaborative teamwork in the clinical workplace.[9] Principles of aviation’s CRM are introduced in a clinical context to model specific applications in the healthcare environment. CTT requires a coordinated, multidisciplinary approach with top leadership engagement and support.[2] The initial implementation of CTT in VHA was optional and included on-site training with integrated simulation conducted by experienced National Center for Patient Safety faculty, followed by coaching and monitoring unit-based safety projects over twelve months. Recurrent training was completed one year from the initial learning session to reenforce key CRM concepts in the program. The fundamental paradigm of CTT is that frontline clinicians are taught specific CRM communication behaviors to manage human error before patients are harmed. The core topics taught within CTT include: the concept of High Reliability, leadership strategies, effective communication, Just Culture and psychological safety, Effective Followership, situational awareness, error tolerance, and then instruction on conducting a local High Reliability Organization (HRO) project.
Human errors are trapped before they reach the patient through effective teamwork, communication, and higher levels of team situational awareness. [10] With the implementation of VHA’s HRO journey in the past 5 years, CTT was required in all clinical areas at each facility and local facility leadership are required to block staff to for attendance. The program used a Train the Trainer model to develop facility-level Master Trainers to implement CTT in 2018. As the implementation spread, NCPS leadership received feedback from the field on multiple challenges in implementing the CTT training and required quality improvement projects. The training started with a video of a poignant patient safety incident involving a routine surgery where complications arose during anesthesia induction. It highlights the tragic consequences of communication failures within the medical team, leading to an inability to adequately address an obstructed airway, ultimately resulting in a preventable death. The following questions were developed to test the participants knowledge and understanding of the principles of Team Training: Who was the leader? What did you think about the communication? What was the team dynamics like? Did they have a sense of urgency or situational awareness? Is this style of leadership Concern for People or Concern for Task? What are the 3 Ws? (What I see, What I’m concerned about, What I think we should do). What are the components that define situational awareness?
Initially, high-level strategic planning meetings between NCPS and the National Center for Organization Development (NCOD) offices were held to discuss reports of local reaction and reception to CTT by VA medical center leadership. More specifically, there were reports of disruptive behavior events being reported during the training and subsequent project implementation of CTT. For example, some clinicians did not think team training would be helpful and did not engage in the training, while other, non-clinicians felt the training was not germane to their work. Consequently, a workgroup within NCPS was formed to: (1) Measure the reaction and reception to CTT training across VA medical centers; (2) Develop a response to any negative reception, including disruptive behaviors to CTT, and (3) Implement and share the developed response(s) to appropriate NCPS leadership and VA medical center leadership.
The multi-professional workgroup was comprised of 11 NCPS team members, including Subject Matter Experts (SMEs) related to CTT, education, analysis, coordination support, and office leadership. Additionally, two NCOD staff were consulted during this program stage to facilitate discussion and guide the development of evaluation and response tools. The multi-professional group met weekly to review CTT materials and known responses from the field. It was decided that further evaluation of the responses from critical VHA medical center staff was needed. A subgroup was formed to host semi-structured focus groups to measure that feedback.
The four focus group facilitators participated in two coaching sessions from NCOD on conducting focus groups. Facilitators were divided into two groups ensuring diversity of backgrounds and facilitation experience. Focus group content was developed iteratively by the subgroup and NCOD consultants with the intent to produce a non-punitive and psychologically safe structured interview to use in the focus groups.
The focus groups targeted VA medical center CTT Points of Contact (POC), HRO Leads and CTT Master Trainers. These positions were thought to have the best exposure and perspective to their local VAMC staff’s reaction and reception to CTT training and project implantation. NCPS sent a request to participate to all VHA CTT POC, HRO Leads, and 60 random CTT Master Trainers from every VA medical center. Forty-eight of the 138 CTT POC and HRO leads (response rate 35%) and 11 of the 60 CTT Master Trainers (response rate 18%) responded. Six of the 48 CTT POC and HRO leads, and 8 of the 11 CTT Master Trainers participated. They were grouped by CTT POC/HRO Lead and CTT Master Trainers, then by date and time preference.
Responses were collected live and presented to all participants in each focus group session to ensure participant comfort and accuracy. All subgroup leaders agreed on iteratively and qualitatively reviewing participant responses from the four open-ended and three poll questions. Each subgroup leader was assigned a question to conduct a preliminary review of participant responses. After the initial review, a second leader then re-reviewed the participant responses. Over multiple iterations, themes emerged and were formalized by the team (see Figure 1 for focus group questions and response themes).
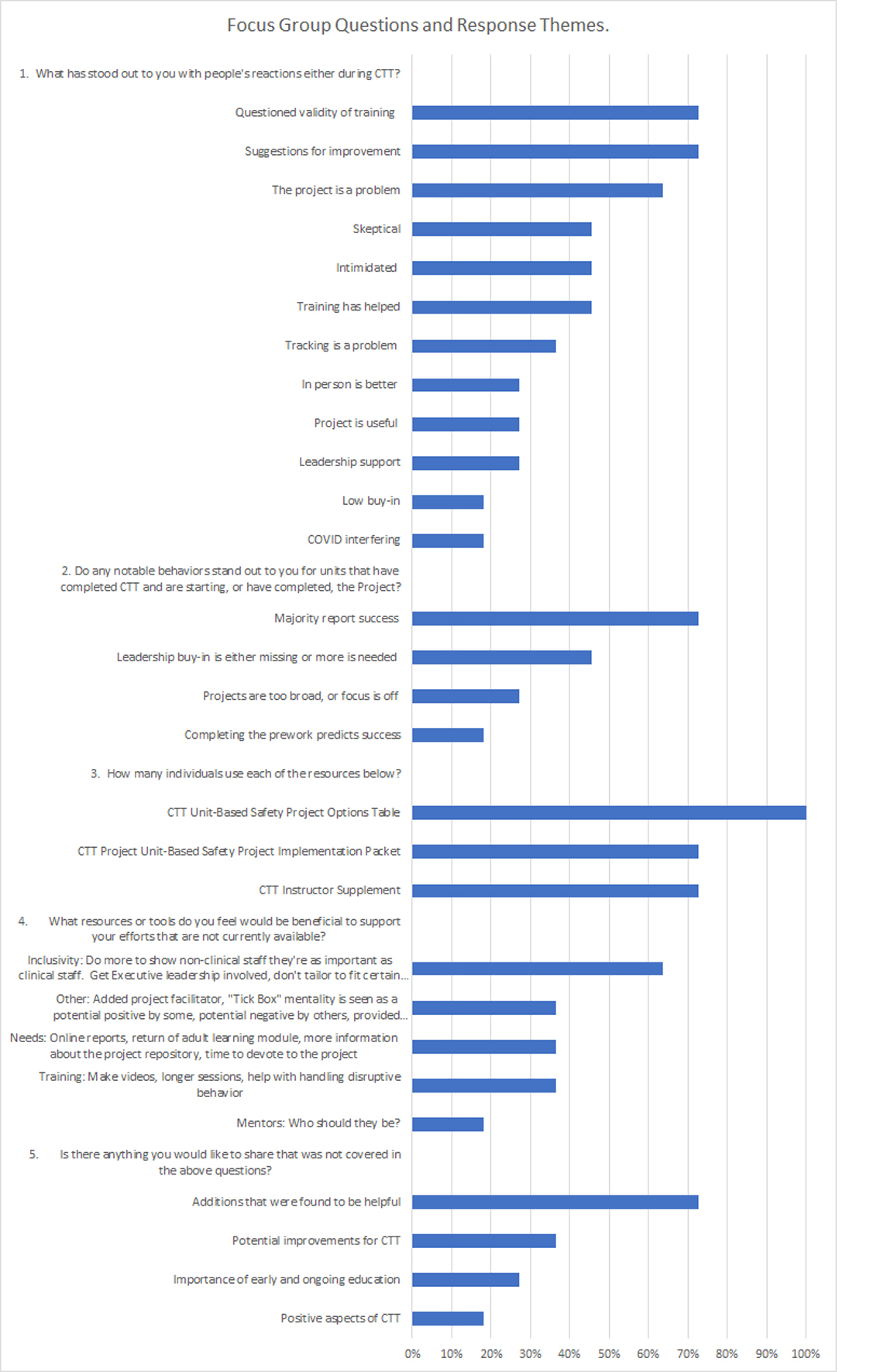
Figure 1.
Focus group questions and response themes
3.Results
Overall, the focus groups revealed that Leadership engagement in cultural change is imperative. The focus groups also identified that language and examples used in the curriculum may have inadvertently marginalized individuals by making some non-clinical team members feel excluded as part of the team. In addition, some participants felt that the use of the term “Projects” created a negative connotation for the required quality improvement project on each unit and instead preferred the terms “micro-project,” “safety strategy,” or “quick wins.”
Table 1 displays the focus group responses by question. Themes are displayed with examples of each theme (see Table 1). For the first question (What, if anything, has stood out to you with people’s reactions either during the teaching of CTT, project selection, or project implementation), the major positive themes were: The training has helped, leadership support is important, and conducting a project is worthwhile. There were also several suggestions for improvement of the program. In addition, the major negative themes included: questions about the validity of the training, problems conducting a project, staff feeling intimidated or overwhelmed, staff feeling skeptical about the training, problems tracking the results, issues with virtual training during the COVID-19 pandemic, and low “buy-in” from staff.
| • Reactions during training- not disruptive behaviors but did have a group brining up unit safety issues thinking master trainers would fix — intent is to give the staff the tools. “People have been respectful” — generally speaking. • The staff that have been trained do understand why we are doing the CTT training. • Reactions re: teaching of CTT-inspiring when they get in the training and see the reality of importance of clinical team interaction-becomes a positive experience. • They do value the content. • We have had folks get so excited they offer to be instructors at the end of the day. |
|
| • The leaders have allowed us to do the CTT training in person. • Leadership was encouraging. • Continued visible leadership support is huge. |
|
| • Most think the project is value-added. • We have trained about 5 units. • I like microproject~, or strategy! OR Unit Based Safety Strategy. |
|
| • Changing the teamwork is important not necessarily numerator/denominator. • We focused on the entire hospital. So we can all be on the same page. • Leadership is also included in this. • We have a full time HRO lead now to help with this. With more marketing now. • We have ELT support. • In QM we are going to be teaching with QM staff and share experiences with training and use that as a marketing tool. • For those that didn't want a face to face we had specific TEAMS invites for them. • We provided nonclinical examples for ancillary staff. • Identifying weaknesses and threats and tying these into the project helps. • Train one team at a time. |
|
| • Making the project mandatory and using a specific tool alienated some staff. • Elaine Bromley video caused strong reactions especially if staff had personal experience losing a patient in this way. Some staff wanted to pick apart the logistics of how the procedure was done rather than looking at the situation r/t HRO. • Leaders making eye contact, as it taught in CTT — can be culturally insensitive, may or may not be appropriate. • ELT member said, “am I not a leader if I don't do all these things?” • Surgery chief told a CTT trainer you are making this all about surgery, like surgeons are the problem. • I've also had some staff say aloud the Effective Followership Algorithm is culturally insensitive. • Comes off as a little out of touch – “this can only be done by front line staff”. |
|
| • May be too much information re: 8 options maybe could be simplified to 1 sheet. • Great reaction to CTT project selection and implementation difficult, sometimes manager decides and implements — staff does not have the time or flexibility in schedules. • Clinicians geared towards tasks — getting them back in room can be difficult for 8 hours. Implementation and sustainment of projects- staff can shut down and do less if they perceive “extra pieces” hard to get ownership. • Staff engagement with projects — OK if staff don’t enter, staff are tired (post Covid) more concerned with implementation rather than completing project. • Perception of “extra work” relating to project. “don’t get the pump primed before they come to CTT” — as in HRO baseline training and other training prior to CTT. |
|
| • Staff willing to do project and are excited until they hear metrics and measurements — not sure what to do with these. • People were intimidated that a project was coming but having a debrief afterward was helpful. • Called a ‘project’ and it's really a “just do it” wish we could have socialized a different term. A year-long makes it seem too long should be i.e., a month. Taking on more energy, (introducing CTT hub) creating an issue “OMG another project and or I am not doing another project, can we count one we are already doing” Frame within the context of implementing one of the strategies of HRO — the way the language is used seems overwhelming. Participants have asked if I fail this is it in my eval? • Ancillary staff felt the clinical material was above their head. • Intimidating to tell group there is a project component. Towards the end the project was more of a positive action. Project component may not be as easy unless you have seen outcomes. |
|
| • Sometimes people think it is “flavor of the month,” as leaders we need to set the expectations it is not “flavor of the month.” • Another common reaction: I love this material, but this is not going to work in our unit due to our leadership. Very common reaction in classes. • There was some pushback especially during COVID. We did a rollout in December of 2020. It has been sustained over time, so people are starting to get that it is important. • Was some discussion about how is this any different than other initiatives? How do we know this is going to work? Is there research on this? We get some research that CTT is in fact effective. • NCPS did CTT for our Surgery team at our facility and the surgery chief told the CTT trainer that he is causing harm today by taking all of us out of surgery. |
|
| • Field experts should be consulted for tracking development. “Deference to expertise” “perfect is the enemy of good.” • It’s the tracking that is problematic. • Message from NCPS is that the front line should enter the tracking data — that may not be the value-added piece. • Most care about work getting done, not data entry. • Project not entered into the hub site for data entry. |
|
| • We have continued to do in person training. • We get more positive feedback when we teach in person. • In this facility they do the training virtually, but there are issues with the virtual training that are open to everyone, so it's hard to track who is trained. |
|
| • Our director just announced that all meetings are going to be virtual, so no face-to-face meeting at this time. We also think face to face it better but it's a challenge. • We explained to execs. And they understand that, but we are having a surge now, so we have a pause in training. |
|
| • Some clinical staff not engaged with material, unusual that nonclinical (finance) very much engaged. • We are not very far in our CTT journey. At the end of January, we have a leadership orientation day for CTT. We are not getting a lot of buy-in. We have staff burn out and staff leaving. |
|
| • Multiple reports of improvement at the VAMC when the unit workgroups engage in the project(s). • Successful projects have no consistent theme, range from: breaking down communication barriers, more collaborative workforce, increase JPSR reporting, GEMBA board use, etc. |
|
| • Leadership presence during the training seems to correlate with successful project engagement in the future. • Projects need sponsorship to gain a foothold, without leadership support many projects flounder. |
|
| • Staff need training on how to refine down the scope, i.e., do PDSAs – projects that fail are always too big • Some projects “get in the weeds,” they don't focus on the project selection from CTT. |
|
| • During CTT training and pre-work, we can generally tell you before the class starts — if the staff are engaged in pre-work, project will be group focused and more successful. Based off engagement of unit. • Prework and teamwork questionnaire can be a predictor of engagement success and sustainment. |
|
| I |
• Also, the nonclinical examples have been helpful. So, all staff could relate, e.g., housekeeping asked what does this have to do with me?” I ask: “what is one thing you got out of this today?” One said: “I matter as a member of the team.” • Have some “high expectation staff” that want everything to be tailored to them — could there be more variability, broader scope. • Staff that are not clinical may not really understand if there are staff outside of clinical use different examples. • Have executive leadership have some interaction/sincere words to show value to the project. • NCPS stresses this is clinical, yet facility staff (nonclinical) are involved, and this is a missed opportunity. – Call it “Critical Team Training” not clinical. Their contributions are just as important as others. • Everyone's goal is HRO – information needs to go to all. This can be missed. Examples are available within group for nonclinical processes too rigid a mindset to say just “clinical.” • Shows staff are all important. Just clinical is a turn-off. |
| • One facility has 3-day training session to develop new CTT instructors, train the trainer for new instructors. Adult learning model. • Videos from NCPS would help, especially the way the trainer talked about using the videos, so you only need one trainer with the videos. Especially during these time with staff leaving or staff having other duties. So, we do not need as many trainers to do the training. We are looking forward to having the videos. • How to handle unruly, disruptive participants should be incorporated into CTT. In many educational programs there are staff that may be negative, and the leaders need tools to turn them around. |
|
| • Needs to be an online version of the “report generator” like NCPS used to generate “TSCQ report,” comparison throughout the nation. Powerful tool, motivational for unit-based projects. TSCQ is written for nurses and physicians, one facility modified it for other staff esp. level 3 sites. • How the national repository for projects is being used would be helpful. What is the purpose? Projects in for 12 months, what are the next steps for new projects for moving forward? • I would also like to see the adult learning module added back in CTT. I'd like to see more alignment with T Coaches and T coaching program. • Make sure staff have time to devote to project. |
|
| • We made a few addition slides on SMART goals, example of issues that could be worked on. • Hired a CTS after CTT launched, has skills for facilitating project work. • I'm concerned CTT projects are at risk of becoming “Tick Box” mentality and losing the focus of culture change. • The CTT repository may nudge toward Tick Box mentality. Selling it would be 50% easier. |
|
| • Question — who should mentor all the staff on these projects is an issue. Can be viewed as a Lean project (some disagree). • Master trainers are expected to be coaches-missed opportunity. Its ok to put master trainers on as mentors. |
|
| • Trainers really liked the situation slide of diagnosis, frequently miss diagnosis. We left that slide in. • Once those who have been through the training start sharing their stories – we are all busy, but people will see that this can help. |
|
| • Written at a much higher level of education than the majority of staff is able to understand and be meaningful. • For front line staff that are overwhelmed — it’s another thing I have to do-need to build a change team-not a fan of “micro project.” • Sustainment can be difficult — need more attention to sustainment, education is a weak action, but certain classes are really important for this to be successful — would like to see this addressed. • Stresses people out when you say project uses “implementation” although it is still a unit-based project. • How do you make safety a byproduct of daily operations — culture change. |
|
| • Because they are called projects, have staff enact the actual strategies instead of focusing on “project, use strategies daily. “Micro projects” -great idea, or “safety strategy” instead of “project” — project has negative connotation. • Not all agree with the renaming as “Micro” project. Rather perhaps “quick wins” Some areas may end up doing a Lean project and can still count as unit-based safety project. • Title and messaging can be helpful, i.e., clinical and project. • Looking at the repository as a positive would be helpful. Selling it would be 50% easier if the word “project” was renewed as a different term. • Tons of resources on national site. “How to facilitate, how to deal with difficult situations….” • Can call a unit project a DOC — “daily operation change” — makes it less stressful. |
|
| • Communicate early and often and take a change-management course. • Get the supervisor involved early. • And planning well ahead of time so there is time. It would be nice to have promotional materials and emails to send to units —for preparation, promotional materials — getting an idea of what it is all about. |
|
For the second question (Do any notable behaviors stand out to you for units that have completed CTT and are starting, or have completed, the Unit-Based Safety Project) the major themes were: The majority reported success, leadership “buy-in” is needed for success, projects can be too broad or the wrong focus. In addition, for the third question, which was a poll on the use of resources supplied by the CTT program, we saw that most of the participants reported using most or all of the resources provided. The resources provided to the field included CTT Instructor Supplement, CTT Project Unit-Based Safety Project Implementation Packet, and CTT Unit-Based Safety Project Options Table (see Table 2).
| CTT Instructor Supplement | 72.7% |
| CTT Project Unit-Based Safety Project Implementation Packet | 72.7% |
| CTT Unit-Based Safety Project Options Table | 100% |
For the fourth question (What resources or tools do you feel would be beneficial to support your efforts in either teaching CTT or facilitating project selection and implementation that are not currently available?), the major themes were: Do more to include nonclinical staff, make more video training, have longer sessions and manage disruptive behavior during training; develop online training, provide more information about conducting the projects, use adult-learning concepts more, provide examples of unit projects, and more information about who the mentors for the project should be.
For the fifth question (Is there anything you would like to share that was not covered in the above questions?), the major themes were: positive aspects of CTT, more suggestions for improvement, and the importance of early and ongoing education about the CCT program to the entire facility.
4.Discussion
The aim of this study was to investigate the implementation of CTT, a well-studied method for promoting the safeguarding of healthcare against unintentional error.[2, 4, 5, 7] The ongoing enterprise-wide implementation of CTT is now mandatory for all VHA staff on clinical units, representing a significant investment of time and resources. Therefore, a thorough evaluation of its effectiveness, impact on patient safety and care outcomes, and the identification of best practices are essential for ensuring a successful and sustainable integration of HRO principles throughout the organization.
Our qualitative investigation provides insights into frontline perceptions of CTT implementation, reinforcing existing literature on barriers to effective team training efforts while also advancing the field with new findings. Specifically, our results support commonly cited required change effort components, including the need for highly visible leadership engagement, adequate time to undertake and complete projects, and overcoming skepticism.[2] For example, successful teams reported having senior leaders addend the training session and provide reasons why the training was important.
CTT master trainers and coordinators noted that a significant barrier to the implementation of the required CTT projects was the term “project” itself. During focus groups, many CTT faculty reported that the term had a negative connotation, given that in the VHA, “project” is usually used in the context of much larger change efforts. To address this hesitancy, teams adopted terms such as “micro-project,” “safety strategy,” or “quick wins,” which were reported as successful methods for overcoming the negative connotation associated with the term.
Team training efforts in the VHA were originally designed based on Medical Team Training, which focused heavily on medical teams. CTT has evolved to expand beyond the narrow focus of medical teams and incorporate a diverse range of clinical, support staff and administrative teams encountered in healthcare organizations. While earlier versions of the training curricula were limited by their clinical focus, CTT has expanded to address this limitation.
The VHA HRO Journey seeks to change cultural norms across the largest integrated healthcare network in the United States, promoting high-quality and safe care for all Veterans who seek care in the VHA. However, achieving cultural change requires more than simply adapting new training tools or materials into the current cultural milieu. It involves transforming and reintegrating mindsets, behaviors, and interactions among individuals and teams within the organization, ultimately leading to a more effective, safety-oriented, and collaborative work environment. Therefore, it is crucial for CTT to impart a lasting impression on how individuals and teams work or respond.
4.1Changes made in VHA as a result of the focus group feedback
The team aggregated the focus group responses and provided the feedback to the larger team developed by NCPS to include the CTT Director. Based on the feedback, the following changes were made. The program’s name has been rebranded to NCPS Team Training, removing the word clinical to be more inclusive of all team members who engage in the care of a patient in the clinical setting. The program developed a complimentary video series for facility Master Trainers to use as a supplement to their teaching or to use the videos exclusively and facilitate the tabletop simulation exercises. Another change is that the Unit Based Safety Project has been renamed as Unit Based Safety Initiative (UBSI) to remove the stigma of a “project.”
4.2Limitations and future directions
This study has several limitations. While qualitative research provides in-depth insights into the perceptions and experiences of participants, it is not easily generalizable to other trainings or populations. Additionally, the focus groups may have been subject to selection bias as they were open to all VHA CTT staff who opted to participate, potentially excluding those who did not have the time or interest in attending. Furthermore, as the study was conducted in a single healthcare system, the generalizability of the findings to other healthcare settings may be limited. Finally, while the study identified barriers to the implementation of CTT, it did not examine the impact of the training on patient safety and care outcomes. Future research could address these limitations by incorporating these findings to drive quantitative exploration of the effort, including a broader range of healthcare systems to improve the generalizability of the findings, and ultimately correlate CTT’s impact on VHA culture and safety outcomes.
In conclusion, this study provides insights into CTT implementation within the VHA healthcare network, highlighting potential barriers to effective team training efforts and strategies for overcoming these barriers. By transforming mindsets, behaviors, and interactions, CTT can play a critical role in promoting a more effective, safety-oriented, and collaborative work environment. To ensure the sustainability and effectiveness of CTT implementation, it is essential to incorporate best practices, evaluate its impact on patient safety and care outcomes, and measure the cultural change it drives within the organization. Ultimately, by adopting a comprehensive approach to cultural change, the VHA can promote high-quality and safe care for all Veterans who seek care in the network.
Authors contributions
Regina Knowles – original concept, writing and editing. Carol M. Jones – writing and editing. Blake Webb, MD – writing and editing. Deborah Welsh, MS – data analysis, writing and editing. Peter D. Mills, PhD, MS – figures, writing and editing, submitting paper for publication.
Ethical statement
Informed patient consent was not required because no patient clinical or identity data was collected, and no patient interventions were completed during the course of study. Therefore ethical review board approval was not required and waived.
Funding
This work has no external financial support.
Conflicts of Interest Disclosure
The author declares that there is no conflicts of interest.
Ethics approval
The Publication Ethics Committee of the Sciedu Press. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
This material results from work supported with resources and using facilities at the Veterans Health Administration National Center for Patient Safety. This is a quality improvement project and not research per Department of Veterans Affairs, Office of Research & Development Program Guide 1200.21, VHA Operations Activities That May Constitute Research, available at
References
- Gross B, Rusin L, Kiesewetter J. Crew resource management training in healthcare: a systematic review of intervention design, training conditions and evaluation. BMJ Open. 2019;9:e025247. PMID:30826798 doi:10.1136/bmjopen-2018-025247
- Ensuring Success and sustainability of quality improvement program. May 13, 2024.
- Veazie S, Peterson K, Bourne D. Evidence Brief: Implementation of High Reliability Organization Principles. Washington (DC); Department of Veterans Affairs (US). 2019. https://www.ncbi.nlm.nih.gov/books/NBK542883/
- Salas E, DiazGranados D, Klein C. Does team training improve team performance? A meta-analysis. Hum Factors. 2008;50(6):903-33. PMID:19292013 doi:10.1518/001872008X375009
- Thomas L, Galla C. Building a culture of safety through team training and engagement. BMJ Qual Saf. 2013;22(5):425-34. PMID:23211280 doi:10.1136/bmjqs-2012-001011
- Frankel A, Leonard M. A Framework for High-Reliability Organizations in Healthcare. Institute of Healthcare Improvement. November 30, 2018. https://www.healthcatalyst.com/learn/insights/high-reliability-organizations-in-healthcare-framework
- Costar D, Hall K. Improving team performance and patient safety on the job through team training and performance support tools: A systematic review. J Patient Saf. 2020;16:S48-S56. PMID:32810001 doi:10.1097/PTS.0000000000000746
- Veterans Health Administration Overview. May 13, 2024. https://www.va.gov/health/#::text=The%20Veterans%20Health%20Administration%20is%20America’s%20largest%20integrated%20health%20care,million%20enrolled%20Veterans%20each%20year
- West P, Sculli G, Fore A. Improving patient safety and optimizing nursing teamwork using crew resource management techniques. J Nurs Adm. 2012;42(1):15-20. PMID:22157377 doi:10.1097/NNA.0b013e31823c17c7
- VHA National Center for Patient Safety Clinical Team Training overview. May 13, 2024. https://www.patientsafety.va.gov/professionals/training/team.asp
 This work is licensed under a
This work is licensed under a 