1.Introduction
Healthcare organizations must consider the means of collecting and disposing of patient bodily waste as part of their overall infection control plan designed to reduce healthcare associated infections (HAIs).[1] Manual washing and disinfecting of bedpans and other vessels pose a risk of exposure to caregivers and the indoor environment via splash and aerosol.[2, 3] Furthermore, manual washing has the potential to leave pathogens residing on the bedpan surface.[1] Bedpans can harbor a wide range of pathogens, including
Very few published studies focus specifically on patient bodily waste management, however hand hygiene is associated with the issues surrounding bodily waste management and health safety. Hand hygiene is a critical component in infection control in healthcare settings. Nurses, being at the forefront of patient care, play a pivotal role in preventing HAIs through proper hand hygiene practices to reduce the incidence of HAIs, therefore reducing the risk of increased morbidity, mortality, and healthcare costs.[7] The Centers for Disease Control (CDC) recommends the use of alcohol-based hand sanitizers (ABHS) for routine hand antisepsis in healthcare settings. Handwashing with soap and water is recommended when hands are visibly soiled or after caring for patients with infectious diarrhea.[8] Despite clear guidelines, compliance with hand hygiene practices among nurses remains a challenge. Workloads and time constraints such as high patient-to-nurse ratios and urgent care demands can limit the time available for proper hand hygiene.[9] Skin dryness and irritation from frequently using ABHS products may discourage consistent practice.[7] Other factors of compliance include lack of readily available hand hygiene products and perceived efficacy.[10, 11]
Hand hygiene disrupts the transmission of pathogens from healthcare workers to patients. By practicing effective hand hygiene, healthcare workers can significantly reduce the transmission of pathogens like MRSA,
In addition to reducing infection rates, improved hand hygiene practices contribute to substantial cost savings. HAIs extend hospital stays and necessitates additional treatments leading to higher healthcare costs. Improving hand hygiene compliance in hospitals could prevent millions of HAIs annually, resulting in savings of $25B to $31.5B in medical costs.[16, 17]
Improved hand hygiene practices contribute to the overall infection control efforts in healthcare facilities. By reducing the reservoir of pathogens on healthcare workers’ hands, the likelihood of environmental contamination is also minimized.[14, 18, 19] A comprehensive approach to infection control enhances safety and quality of patient care.[7] Patient bodily waste management is part of that comprehensive approach. Having the proper tools and education for managing patient waste will improve infection prevention efforts in healthcare systems. Studies should be conducted to ascertain the impact of improved practices for patient bodily waste management to discern the value, both in terms of reducing risk of infection and cost implications.
Another related topic of concern is needlestick injuries (NSIs). NSIs are classified as a significant occupational hazard in healthcare settings, causing risks of transmission of bloodborne pathogens such as hepatitis B virus, hepatitis C virus, and human immunodeficiency virus. Occupational NSIs are common in healthcare facilities, affecting a significant proportion of healthcare workers. One study estimated that approximately 2 million healthcare workers experience NSIs annually leading to a substantial number of infections with bloodborne pathogens.[20] Factors contributing to NSIs include high patient-to-staff ratios and long working hours leading to fatigue and lapses in concentration, increasing the likelihood of an error; insufficient training on the proper handling and disposal of sharps can result in accidental injuries; and the absence of safety-engineered devices, such as needleless systems and safety syringes.[3, 20, 21, 22, 23] Like patient bodily waste management, ongoing education, the use of safety-engineered devices, and comprehensive infection control protocols are essential to protect healthcare workers from needlestick injuries and their potentially serious consequences.
Patient bodily waste management impacts nurses, other healthcare workers, and the healthcare organization. For nurses and other healthcare workers, the risk of exposure to pathogens can have adverse health effects, increase stress, and reduce work satisfaction, potentially leading to retention issues.[24, 25, 26] Proper training and using safety-engineered devices to reduce exposure risks and improve shorter bedside toileting, may reduce stress, and improve work satisfaction.[27] Reducing risk of exposure reduces HAI risk of patients, nurses, and other healthcare workers, reducing the cost of care for organizations.[4, 5, 28]
2.Methods
2.1Subject selection & recruitment
The subject population targeted for the research was nursing professionals filling a variety of nursing roles requiring an associate, bachelor, or advanced nursing degree. The American Nurses Association (ANA) database is a membership listing of professional nurses which was used for recruitment by nurse type, practice setting, specialty, and academic degree. Additionally, recruitment included participants at professional conferences such as Association of Professionals of Infection Prevention and The American Nurses Credentialing Center National Magnet Conference, mailing lists of nurses and infection preventionists, and participants in continuing education presentations. No population within the professional nurse inclusion criteria were excluded from participation. No vulnerable populations are included in this study. All participants were of working age, 18 years and older. An exemption from IRB review was provided by Baylor University Institution Review Board on June 22, 2023.
The study was anonymous, and, through the recruitment process, no emails were recorded. Consent was obtained and the survey was provided in Spanish and English according to the IRB Exempt protocol. For those who started and did not complete the survey, their responses remained in the data and were used in the analysis. Questions that were not answered were reported as missing data. None of the participants withdrew from the study nor asked to be removed from the data set. Undue influence or coercion was minimized by making an anonymous solicitation. The opportunity to participate was squarely in the potential participant’s corner. The researchers did not have access to emails for those who decided not to participate. Researchers did not have access to emails for those who participated and responded in any way. This is not a randomized selection list; rather the selection is driven by finding participants in professional settings.
2.2Research design and method
The purpose of this project was to gain insight into nursing needs, perceptions, and satisfaction related to patient bodily waste management. The hypothesis for this study was that healthcare organizations have systems in place for the safe elimination of bodily waste management and nurses are knowledgeable of the risks and utilize resources provided to maintain a safe working environment. To that end, the following are the aims of the study:
Aim 1: Knowledge and Level of Exposure. The survey assessed nurse knowledge about the risks of exposure to non-blood bodily material and the level of those exposures.
• Sub Aim: The evaluation of the data determined if there were differences in knowledge and perceptions based on type of hospital and other demographic factors.
Aim 2: Procedures and Reporting. The survey assessed the level of reporting and current procedures to mitigate impacts of exposures to non-blood bodily material.
• Sub Aim: The evaluation of the data determined if there were differences in procedures and reporting based on type of hospital and other demographic factors.
Aim 3: Satisfaction and Morale. The survey assessed nurses’ current levels of satisfaction and morale with how risks of exposure to non-blood bodily material were currently managed.
• Sub Aim: The evaluation of the data determined if there are differences in satisfaction and morale based on type of hospital and other demographic factors.
The methodology of this study utilized a survey with a quantitative design. The survey was developed specifically for this inquiry. The first set of questions aligned with Aim 1 and focused on knowledge about the risk and their personal level of exposure. The second set of questions aligned with Aim 2 and focused on the participant’s understanding of procedures and incident reporting. The next set of questions aligned with Aim 3 and focused on morale and satisfaction with their job. The final set of questions were demographic questions intended to be used as dependent variables for analysis. The demographic questions encompassed variables such as age, gender, and the number of years a nurse had been employed in the healthcare sector. Additional inquiries pertained to the type of healthcare facility (e.g., community hospital, university hospital), the facility’s size as determined by bed count, and its geographical location (e.g., rural, suburban, urban). In this study, rural areas are defined as regions with low population density and extensive open spaces primarily dedicated to agriculture and natural resource-based industries. Urban areas are characterized by high population density and a significant concentration of infrastructure, businesses, and cultural amenities. Suburban areas are described as a blend of rural and urban environments, featuring residential neighborhoods near urban centers that provide access to city amenities and open spaces.
This area of inquiry is understudied and has limited research in literature. However, the literature on this topic and related topics (e.g., needle stick injuries and hand hygiene) contributed to the development of the survey questions. Review of the survey was conducted by an expert in the field and a pilot study assessed the questions to get additional input from those who are most affected by management of bodily waste.
A pilot survey was shared with ten potential respondents who were not part of the selection cohort but had an interest in the topic. The purpose of the pilot study was to assess the veracity of the questions and determine if there were any obstacles for participants to complete the survey. Seven participants completed the pilot survey. The data and open comments were analyzed and reviewed. Based on several added comments for the pilot study, all agreed that there were no questions that could not be answered given the choices provided and no additional topics or questions should be added to the survey. The composition of the survey remained unchanged. After the completion of the analysis of the pilot survey, the survey was released. Since no personal information was collected and participation was voluntary, the risk of bias was minimized. The survey was available to the participants for approximately three weeks in both English and Spanish languages. Data collection took place during the 2023 calendar year after IRB Exempt approval. The survey was administered in electronic format using Qualtrics.[29]
2.3Analysis
Primary aims were addressed using descriptive statistics, proportions in categories of responses. For sub aims, to determine if there were significant differences across groups, either a Pearson’s Chi-squared test or Fisher’s exact test were run. The Fisher’s exact test was run only if the assumptions for the expected counts of a Chi-squared test were not met, specifically for gender and whether the facility is a Magnet facility for specific questions. A Magnet hospital is a healthcare organization recognized for excellence in nursing services and adherence to high standards of patient care.[30] The cutoff point to determine significance was set to alpha = 0.05. For text answer questions, we tokenized responses, removed stop words, and used stemming to avoid duplicates of words. Graphical methods were utilized to display results for all analysis as appropriate. All computations were done in the statistical software program R, version 4.1.1[31] and for text data using the “textdata” package.[32]
3.Results
3.1Demographics
Of those who provided consent to participate (
| 20 or under | 2 (0.8%) |
| 21-29 | 14 (5.3%) |
| 30-39 | 67 (25%) |
| 40-49 | 61 (23%) |
| 50-59 | 58 (22%) |
| 60 or over | 64 (24%) |
| Female | 237 (89%) |
| Male | 26 (9.8%) |
| Prefer to self-describe | 2 (0.8%) |
| 0-5 | 17 (6.4%) |
| 5-10 | 32 (12%) |
| 10-15 | 50 (19%) |
| 15-20 | 48 (18%) |
| 20 or more | 119 (45%) |
| 0-5 | 93 (35%) |
| 5-10 | 60 (23%) |
| 10-15 | 51 (19%) |
| 15-20 | 29 (11%) |
| 20 or more | 30 (11%) |
| Community hospital | 147 (56%) |
| Federal government hospital | 16 (6.1%) |
| Other | 66 (25%) |
| University hospital | 33 (13%) |
| Rural | 52 (20%) |
| Suburban | 95 (36%) |
| Urban | 114 (44%) |
| Large hospital: 500 or more beds | 67 (26%) |
| Medium hospital: 100 to 499 beds | 132 (52%) |
| Small hospital: Fewer than 100 beds | 56 (22%) |
| No | 177 (69%) |
| Yes | 80 (31%) |
| No | 174 (69%) |
| Yes | 77 (31%) |
| Advanced Practice Registered Nurse (APRN) | 7 (2.6%) |
| Certified Nurse Assistant (CNA) | 2 (0.8%) |
| Certified Nurse Educator (CNE) | 1 (0.4%) |
| Clinical Nurse Specialist (CNS) | 5 (1.9%) |
| Infection Preventionist (IP) | 65 (25%) |
| License Practical Nurse (LPN) | 3 (1.1%) |
| Nurse Practitioner (NP) | 9 (3.4%) |
| Other | 13 (4.9%) |
| Registered Nurse (RN) | 160 (60%) |
| Cardiac Catheterization Laboratory | 2 (0.8%) |
| Cardiac/Coronary Care | 5 (1.9%) |
| General Practice | 26 (10%) |
| Geriatrics | 21 (8.1%) |
| Intensive Care | 19 (7.3%) |
| Medical-Surgical | 43 (17%) |
| Neurological Intensive Care | 2 (0.8%) |
| Orthopedics | 5 (1.9%) |
| Other | 124 (47%) |
| Pediatrics | 13 (5.0%) |
3.2Knowledge about risk of exposure
Nurse responses to survey questions about their knowledge of risk exposure indicated high agreement (see Table 3).
| Management of waste is important | 11 (4.1%) | 2 (0.8%) | 4 (1.5%) | 24 (9.0%) | 225 (85%) |
| Exposures desensitize workers to risks | 19 (7.1%) | 22 (8.3%) | 10 (3.8%) | 90 (34%) | 125 (47%) |
| Containment can decrease cost | 5 (1.9%) | 6 (2.3%) | 13 (4.9%) | 72 (27%) | 169 (64%) |
| Concern: needle stick | 4 (1.5%) | 16 (6.0%) | 19 (7.2%) | 97 (37%) | 129 (49%) |
| Concern: blood splash | 4 (1.5%) | 13 (4.9%) | 27 (10%) | 112 (43%) | 107 (41%) |
| Concern: stool splash (eyes/nose/mouth) | 3 (1.2%) | 19 (7.4%) | 25 (9.7%) | 109 (42% | 102 (40%) |
| Concern: stool splash (skin) | 4 (1.5%) | 28 (11%) | 37 (14%) | 106 (41%) | 85 (33%) |
Respondents had high agreement that:
- Management of patient bodily waste is important (94%).
- Responsible containment using waste management devices can decrease costs of HAI (91%).
- Repeated exposure desensitizes healthcare workers to risks (81%).
When considering risk associated with exposures to patient bodily waste:
- Needle stick injury was considered the highest risk (86%).
- Blood and stool splash/spills to the eye, nose, or mouth was considered high risk (83%).
- Stool splash/spills on skin or clothing was considered high risk by 73% of respondents.
For the question, “How concerned are you about the risk associated with blood splash/spill exposures (low risk to high risk)?” gender (see Figure 1) and age were significantly different (
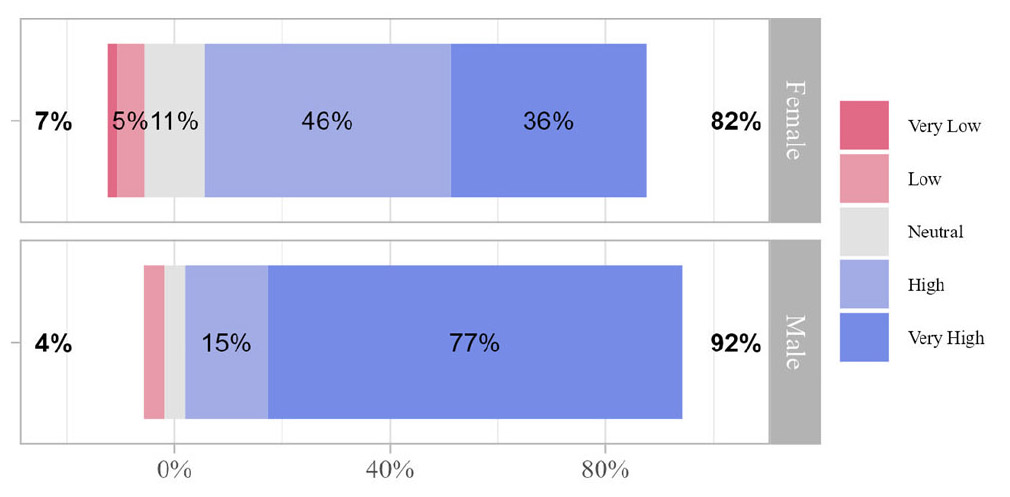
Figure 1.
Nurses’ concern about the risk associated with patient bodily waste exposures
Type of facility and urban/suburban/rural facility were significantly different for “How concerned are you about the risk associated with stool splash/spill to the eyes, nose, and mouth during cleaning (low risk to high risk)?” were significantly different (
3.3Procedures and reporting
For questions focusing on organizational procedures, an interesting pattern emerged showing that knowledge of procedures did not align with follow-through of reporting; and similar results indicating that while PPE is available, nurses typically only use gloves (see Table 4). Eighty-eight percent of respondents responded that they did not report stool splash or spill events despite 76% agreeing that their hospital has clear and easy reporting methods. The respondents overwhelmingly feel they would need to “justify” such a report.
| Would feel need to justify actions | 35 (13%) | 25 (9.4%) | 31 (12%) | 105 (40%) | 69 (26%) |
| Hospital has clear reporting methods | 7 (2.7%) | 24 (9.2%) | 33 (13%) | 97 (37%) | 101 (39%) |
| Reporting Frequency: | |||||
| Stool splash (eyes/nose/mouth) | 119 (84%) | 12 (8.5%) | 2 (1.4%) | 2 (1.4%) | 6 (4.3%) |
| Stool splash (skin/clothes) | 124 (78%) | 24 (15%) | 3 (1.9%) | 3 (1.9%) | 5 (3.1%) |
| Mitigation Measures Implemented: | |||||
| Plan gap with meals | 117 (46%) | 34 (13%) | 30 (12%) | 40 (16%) | 34 (13%) |
| Protection disposing sharps | 7 (2.7%) | 15 (5.8%) | 9 (3.5%) | 51 (20%) | 177 (68%) |
| Protection cleaning bedpans | 13 (5.1%) | 26 (10%) | 13 (5.1%) | 45 (18%) | 157 (62%) |
| Gloves | 0 (0%) | 2 (0.8%) | 0 (0%) | 14 (5.4%) | 245 (94%) |
| Face Mask | 38 (15%) | 94 (37%) | 25 (9.7%) | 35 (14%) | 65 (25%) |
| Face Shield | 88 (35%) | 90 (35%) | 22 (8.6%) | 22 (8.6%) | 33 (13%) |
| Gown or Apron | 30 (12%) | 93 (36%) | 30 (12%) | 40 (16%) | 64 (25%) |
| Respirator | 144 (57%) | 83 (33%) | 4 (1.6%) | 8 (3.2%) | 12 (4.8%) |
| Goggles | 109 (43%) | 89 (35%) | 17 (6.8%) | 12 (4.8%) | 24 (9.6%) |
| Macerators | 202 (80%) | 39 (15%) | 12 (4.7%) | ||
| Bedpan Liners | 162 (63%) | 27 (11%) | 68 (26%) | ||
| Splash Screens | 175 (68%) | 22 (8.5%) | 62 (24%) | ||
| Bedpans | 101 (39%) | 64 (24%) | 97 (37%) |
When asked which of the following mitigation mechanisms and devices has your hospital implemented (macerators, bedpan liners, splash screens, and bedpan or urine bottle management), the response suggested lack of implementation of mitigation methods.
Three questions focused on actions taken by the respondents to mitigate their own risk.
- Only 29% of respondents consider the impact of exposures close to meal breaks.
- Eighty percent of nurses use PPE, although 99% only use gloves.
Agreement for the following statements were significantly different by gender (see Table 5 and Figure 2).
| Investing fosters job satisfaction. | 2 (0.8%) | 0 (0%) | 26 (9.8%) | 85 (32%) | 153 (58%) |
| Investing improves nurse retention. | 0 (0%) | 3 (1.1%) | 65 (24%) | 81 (30%) | 117 (44%) |
| Utilizing containment improves the quality of patient care. | 2 (0.8%) | 2 (0.8%) | 25 (9.4%) | 81 (30%) | 156 (59%) |
| Containment solutions positively impact healthcare worker dignity. | 2 (0.8%) | 3 (1.1%) | 19 (7.1%) | 64 (24%) | 178 (67%) |
| How satisfied are you with the current protocol? | 18 (6.8%) | 60 (23%) | 82 (31%) | 79 (30%) | 25 (9.5%) |
| What is your level of stress while performing bodily waste tasks? | 12 (4.6%) | 77 (30%) | 112 (43%) | 47 (18%) | 11 (4.2%) |
| What is your level of anxiety while performing bodily waste tasks? | 19 (7.3%) | 85 (33%) | 111 (43%) | 35 (14%) | 9 (3.5%) |
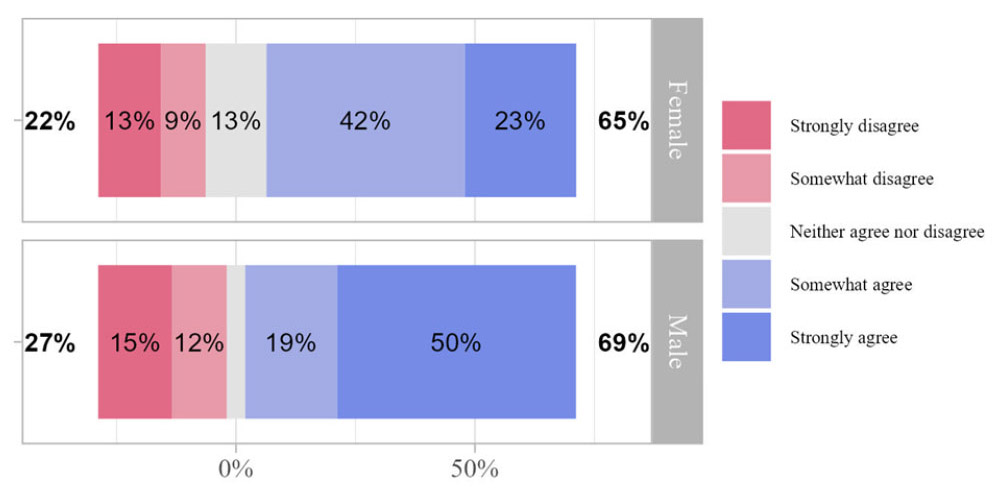
Figure 2.
Nurses who feel the need to justify their actions if an incident report was made for a needle stick, blood splash or spill, or stool splash or spill by gender
- “I would feel the need to justify my actions if I were to make an incident report for needle stick, blood spill or splash, or stool spill or splash” (
p = .023). Male nurses were more concerned with justification of their actions then female nurses. - “My hospital has implemented regular self-reporting checklists and tools for compliance with procedures when manually cleaning bedpans” (
p = .010). Female nurses had more confidence in their processes and procedures than male nurses. - “My hospital has adequate engineering controls such as ventilation, equipment, and protective barriers for reducing hazards from coming into contact with healthcare workers” (
p = .049). Male nurses indicated more confidence in their facility engineering controls than female nurses.
The question “In the past 3 months, how often did you report a... blood splash or spill?” was significantly different by age and years of experience (
The question “In the past 3 months, how often did you report a... needle stick injury?” was significantly different by type of facility and magnet facility (
The statement, “My hospital has adequate engineering controls such as ventilation, equipment, and protective barriers for reducing hazards from coming into contact with healthcare workers” was significantly different by the size of the facility with
For magnet facilities, the statements “My hospital has implemented regular self-reporting checklists and tools for compliance with procedures when manually cleaning bedpans” and “My hospital has adequate engineering controls such as ventilation, equipment, and protective barriers for reducing hazards from coming into contact with healthcare workers” were significant (
4.Nurse satisfaction and morale
There was strong agreement among nurses with the role that managing patient bodily waste plays in morale and satisfaction (89%), nurse retention (74%), healthcare worker dignity (91%), and quality of patient care (89%) (see Table 5).
While the respondents recognize its importance, 39% were satisfied with the current protocols in their workplace for managing bodily waste. Only 22% reported stress and 17% reported anxiety when performing these tasks.
When asked about the level of personal stress or anxiety while performing tasks associated with patient bodily waste as a part of your job as a healthcare worker, both were significantly different by age (see Figure 3) (
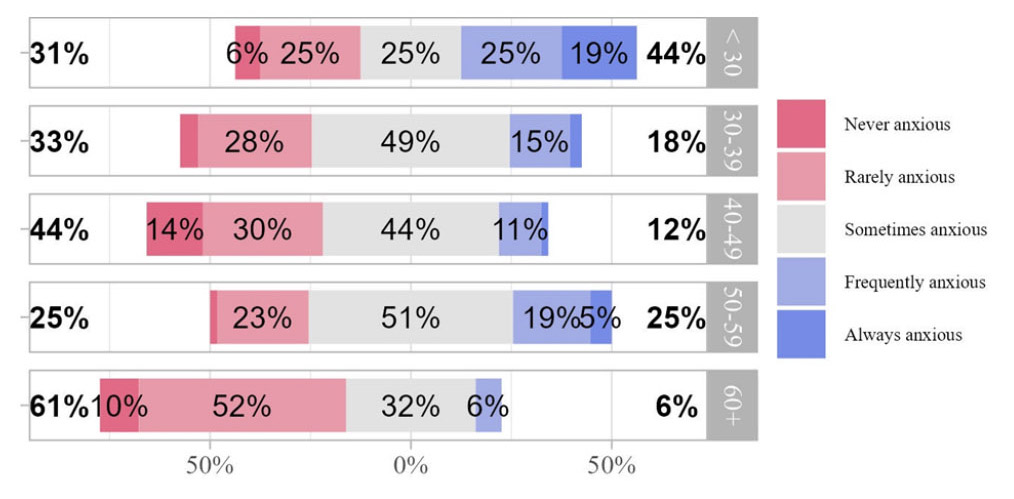
Figure 3.
Nurses report levels of anxiety while performing tasks associated with patient bodily waste as a part of the healthcare worker job by age
For facility size (see Table 6), the statement, “Investing in best nursing practices for patient bodily waste management improves nurse retention” had a
| Extremely inadequate | 6 (9.1%) | 6 (4.5%) | 4 (7.1%) | |
| Somewhat inadequate | 15 (23%) | 18 (14%) | 9 (16%) | |
| Neither adequate nor inadequate | 14 (21%) | 17 (13%) | 12 (21%) | |
| Somewhat adequate | 15 (23%) | 68 (52%) | 21 (38%) | |
| Extremely adequate | 16 (24%) | 23 (17%) | 10 (18%) | |
| Unknown | 1 | 0 | 0 | |
| Strongly disagree | 0 (0%) | 0 (0%) | 0 (0%) | |
| Somewhat disagree | 1 (1.5%) | 0 (0%) | 1 (1.8%) | |
| Neither agree nor disagree | 18 (27%) | 35 (27%) | 11 (20%) | |
| Somewhat agree | 13 (19%) | 37 (28%) | 27 (48%) | |
| Strongly agree | 35 (52%) | 60 (45%) | 17 (30%) | |
Nurses agreed that “investing in best nursing practices for patient bodily waste management fosters a culture of job satisfaction.” and for the question, “what is your level of anxiety while performing tasks associated with patient bodily waste as a part of your job as a healthcare worker?” nurses working for Pathway to Excellence facilities reported more anxiety compared to nurses at other hospitals (
| Strongly disagree | 1 (0.6%) | 1 (1.3%) | |
| Somewhat disagree | 0 (0%) | 0 (0%) | |
| Neither agree nor disagree | 13 (7.5%) | 11 (14%) | |
| Somewhat agree | 67 (39%) | 13 (17%) | |
| Strongly agree | 93 (53%) | 52 (68%) | |
| Never anxious | 12 (7.1%) | 7 (9.1%) | |
| Rarely anxious | 63 (37%) | 18 (23%) | |
| Sometimes anxious | 74 (44%) | 31 (40%) | |
| Frequently anxious | 15 (8.8%) | 18 (23%) | |
| Always anxious | 6 (3.5%) | 3 (3.9%) | |
| Unknown | 4 | 0 | |
5.Discussion
The safe disposal of patient bodily fluids or waste typically falls within the realm of nursing responsibilities, impacting not only their personal safety but also influencing the well-being of patients and the financial health of the healthcare organization. Body fluids are defined as blood, feces, urine, vomit, saliva, semen, vaginal secretions, and any other fluids that originate from a human body.[34] Materials tainted with blood or bodily fluids, as well as waste from patients, may be infectious, elevating the risks of exposure. Nurses expressed a strong consensus regarding the significance of managing bodily waste in patient care. Furthermore, repeated encounters with spills and splashes of bodily waste can desensitize healthcare workers to the associated risks. Finally, employing proven waste management strategies for responsible containment has the potential to reduce costs, improving fiscal management of the organization. Utilizing a bodily waste system designed to protect both patients and healthcare workers may, in turn, diminish the risk of HAIs.
Evaluating the risk associated with blood splashes and spills, a notable contrast emerged: a higher percentage of males (77%) expressed an elevated level of concern compared to females (36%). It is worth noting however, that male participants constitute less than 10% of the total sample (
Accidental splashes or spills of patient bodily waste can increase the risk of exposure to contaminated materials and surfaces. Healthcare systems have procedures that require reporting, clean-up, decontamination, and disposal of bodily waste spills. The data shows that needle stick injury and stool splash or spill during cleaning effecting the eyes, nose, or mouth were the least experienced incident types, while blood splash or spill and stool splash or spill during cleaning effecting skin or clothing showed increased incidents impacting respondents. However, a high percentage of these same respondents indicated that they did not report these events, despite being aware and agreeing that their hospital system has clear and easy reporting methods, stating that a justification for the reporting was a determining factor in not reporting. Those reporting incidents were likely to be the younger (< 30) and older nurses (> 50). Underreporting is expected, but by not reporting, the commitment to develop policy and procedures to improve the outcomes are less likely.
While males were more likely to respond that controls and methods in place were adequate, but they were also more likely to have a higher level of concern about the risk and felt the need to justify reporting an incidence. Hospitals recognized as Magnet facilities were more likely to report or have implemented controls and procedures to support mitigation through reporting and engineering controls, which may lead to improved nurse satisfaction. Overall, nurse responses to the type of devices that have been implemented by one’s organization suggest a gap between nurse perceived risk of exposure and a lack of implementation of mitigation strategies such as the use of macerators, bedpan liners, splash screens, and bedpan or urine bottle devices.
Personal protective equipment (PPE) is equipment, such as gloves, safety glasses or face shields, shoe covers, respirators, and gowns or coveralls worn to minimize exposure to hazards that cause serious workplace injuries and illnesses.[18] Nurses in this study use PPE for personal protection when performing bodily waste management tasks, however, 99% consistently use only gloves. While healthcare organizations have policies and procedures in place, individual choice of nurse professionals suggests that organizational expectations of reporting incidents and utilizing PPE for personal safety are not being met. By not providing the necessary information, nurses may prevent opportunities to make productive changes to mitigate risks.
Satisfaction, morale, and dignity are crucial elements in maintaining a healthy and thriving nursing profession.[24, 26] These factors contribute not only to the well-being of individual nurses but also to the overall quality of patient care and the healthcare system. Ensuring a safe and healthy work environment preserves the dignity of nurses. Adequate staffing levels, proper equipment, and measures to prevent workplace injuries and illnesses contribute to a workplace that increases satisfaction and morale.
Respondents to the nurse survey showed strong agreement with the role of managing patient bodily waste in morale and satisfaction. Nurses perceive that investing in best nursing practices fosters a culture of job satisfaction and improves nurse retention, especially nurses from large facilities. Nurses also perceive that utilizing containment devices such as bedpan washer shields and liners to minimize risk exposure improves the quality of patient care and positively impacts healthcare workers’ dignity. However, nurses were not satisfied with the current controls and protocols in their workplace for handling patient bodily waste. As a function of their job, 47% of nurses have some level of stress associated with performing tasks associated with patient bodily waste with younger respondents and those employed at Pathway to Excellence facilities reporting higher levels of stress and anxiety. While nurses face a variety of challenges, understanding the risks and the opportunity for improved procedures and devices about patient bodily waste management is a factor that can improve morale and nurse satisfaction, and contribute to a stable workforce.
This study relied on responses from participants who are credentialed nurses. A potential limitation is response bias where participants may provide dishonest or socially desirable answers rather than their true opinions leading to biased results. This study had only two open-ended responses that contribute to the narrative described in this manuscript. An imbalance in the demographics made some comparisons challenging. For instance, there were significant differences based on gender, but the percentage of male participants was low when compared with the female participants.
For organizations to retain and recruit quality nursing professionals, policies and procedures must be in place to support quality patient care while protecting the health and safety of healthcare workers, including nurses. Empowering nurses to contribute to a better understanding of the challenges and potential improvements in patient bodily waste management are likely to increase satisfaction and morale, leading to improved patient care outcomes and a stronger healthcare system.
Recommendations for improving management of bodily waste in hospitals
1. There is a need for the development of public health efforts to integrate programs to enhance knowledge and practices of healthcare workers to better control the spread of multidrug-resistant bacteria with comprehensive infection control programs.
2. A comprehensive approach to infection control, including hand hygiene, needlestick injury, and patient bodily waste management will enhance safety and quality of patient care while providing a safe work environment.
3. Proper training and using safety-engineered devices to reduce exposure risks, improve shorter bedside toileting, reduce stress, and increase work satisfaction. Investing in a patient bodily waste management system fosters a culture of job satisfaction.
4. Utilizing proven waste management strategies for responsible containment has the potential to reduce costs, improving fiscal management of the organization. Utilizing a bodily waste system designed to protect both patients and healthcare workers may, in turn, diminish the risk of HAIs.
5. Encourage use of recommended PPE for personal safety to reduce incidents of exposure and mitigate risk.
6. Encourage incident reporting. Remove the fear of retribution. Support nurses so that when problems arise, policy and procedures can be amended to improve outcomes.
7. Ensuring a safe and healthy work environment preserves the dignity of nurses. Adequate staffing levels, proper equipment, and measures to prevent workplace injuries and illnesses contribute to a workplace that increases satisfaction, morale, and contributes to a stable workforce.
Authors contributions
Conceptualization, D.H. and R.X.S.; methodology, D.H. and R.X.S.; validation, R.X.S and A.K. formal analysis, R.X.S and A.K. investigation, D.H. and R.X.S.; resources, D.H. and R.X.S.; data curation, D.H., A.K. and R.X.S.; writing—original draft preparation, D.H., A.K. and R.X.S.; writing—review and editing, D.H. and R.X.S.; visualization, D.H., A.K. and R.X.S.; supervision, D.H. and R.X.S.; project administration, D.H. and R.X.S.; All authors have read and agreed to the published version of the manuscript.
Ethical statement
Informed patient consent was not required because no patient clinical or identity data was collected, and no patient interventions were completed during the course of study. Therefore ethical review board approval was not required and waived.
Funding
was provided by Cleanis, Inc.
Conflicts of Interest Disclosure
The author declares that there is no conflicts of interest.
Ethics approval
The Publication Ethics Committee of the Sciedu Press. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Data sharing statement
No additional data are available.
Acknowledgements
The authors would like to thank Cleanis, Inc. for providing the funding for this study. The topic of nurse and healthcare worker safety and patient quality of care is always important, but this specific topic is under researched.
References
- Apple M. Toward a Safer and Cleaner Way: Dealing With Human Waste in Healthcare. HERD. 2016;9(4):26-34. PMID:26747841 doi:10.1177/1937586715619739
- van Knippenberg-Gordebeke G. Bedpan management, part of healthcare waste management. Journal of Patient Safety & Infection Control. 2015;3(2):32-33. doi:10.1016/j.jpsic.2015.10.204
- Goss L. Splashes & Sharps: Occupational Exposures in the Health Care Setting. Occupational Health & Safety. 2015;84(4):42-46.
- van Knippenberg-Gordebeke G. P376: Dirty bedpans and MDRO: partners in crime? Antimicrobial resistance & Infection Control. 2013;2:376-376. doi:10.1186/2047-2994-2-S1-P376
- Shams A, Rose L, Edwards J. Assessment of the Overall and Multidrug-Resistant Organism Bioburden on Environmental Surfaces in Healthcare Facilities. Infect Control Hosp Epidemiol. 2016;37(12):1426-1432. PMID:27619507 doi:10.1017/ice.2016.198
- N’Guyen T, Bourigault C, Guillet V. Association between excreta management and incidence of extended-spectrum . Journal of Hospital Infection. 2019;102(1):31-36. PMID:30557588 doi:10.1016/j.jhin.2018.12.006
- Tartari E, Bellissimo-Rodrigues F, Pires D. Updates and future directions regarding hand hygiene in the healthcare setting: insights from the 3rd ICPIC alcohol-based handrub (ABHR) task force. Antimicrobial Resistance & Infection Control. 2024;13(1):26-26. PMID:38424571 doi:10.1186/s13756-024-01374-9
- CDC. Clinical Safety: Hand Hygiene for Healthcare Workers. February 27, 2024. https://www.cdc.gov/clean-hands/hcp/clinical-safety/index.html
- Pittet D, Hugonnet S, Harbarth S. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Infection Control Programme. Lancet. 2000;356(9238):1307-12. PMID:11073019 doi:10.1016/S0140-6736(00)02814-2
- Stone P. Economic burden of healthcare-associated infections: an American perspective. Expert Review of Pharmacoeconomics & Outcomes Research. 2009;9(5):417-422. PMID:19817525 doi:10.1586/erp.09.53
- Erasmus V, Daha T, Brug H. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infection Control and Hospital Epidemiology. 2010;31(3):283-294. PMID:20088678 doi:10.1086/650451
- Apisarnthanarak A, Ratz D, Khawcharoenporn T. National Survey of Practices to Prevent Methicillin-Resistant Staphylococcus aureus and Multidrug-Resistant Acinetobacter baumannii in Thailand. Clin Infect Dis. 2017;64:S161-S166. PMID:28475783 doi:10.1093/cid/cix045
- WHO. Scientific Brief. World Health OrganizationGeneva, Switzerland. 2020.
- Wu S, Wang Y, Jin X. Environmental contamination by SARS-CoV-2 in a designated hospital for coronavirus disease 2019. Am J Infect Control. 2020;48(8):910-914. PMID:32407826 doi:10.1016/j.ajic.2020.05.003
- Larson E, Early E, Cloonan P. An Organizational Climate Intervention Associated With Increased Handwashing and Decreased Nosocomial Infections. Behavioral Medicine (Washington, D.C.). 2000;26(1):14-22. PMID:10971880 doi:10.1080/08964280009595749
- Scott R. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. D. o. H. Q. Promotion, e.d. Centers for Disease Control and Prevention. 2009.
- Ojanperä H, Kanste O, Syrjala H. Hand-hygiene compliance by hospital staff and incidence of health-care-associated infections, Finland. Bulletin of the World Health Organization. 2020;98(7):475-483. PMID:32742033 doi:10.2471/BLT.19.247494
- Barr K, Sturdivant R, Williams D. Bacteria Associated with Healthcare-Associated Infections on Environmental Samples Obtained from Two Fire Departments. International Journal of Environmental Research and Public Health. 2021;18(22):11885. PMID:34831638 doi:10.3390/ijerph182211885
- Harris D, Taylor K, Napierkowski K. Indoor Finish Material Influence on Contamination, Transmission, and Eradication of Methicillin-Resistant Staphylococcus aureus. Health Environments Research & Design. 2020;14(1):118-129. PMID:32867539 doi:10.1177/1937586720952892
- Mazi W, Senok A, Assiri A. Occupational exposure to blood-borne pathogens in a tertiary hospital: benchmarking using patient days. Asia Pac J Public Health. 2015;27(2):NP1727-32. PMID:22743860 doi:10.1177/1010539512450608
- Centers for Disease Control and Prevention. NIOSH Safety and Health Topic: Health Care Workers. November 27, 2011. http://www.cdc.gov/niosh/topics/healthcare/
- Hersey J, Martin L. Use of infection control guidelines by workers in healthcare facilities to prevent occupational transmission of HBV and HIV: results from a national survey. Infect Control Hosp Epidemiol. 1994;15(4):243-52. PMID:8207191 doi:10.1086/646904
- Kennedy M, O’Reilly D, Mah M. The use of a quality-improvement approach to reduce needlestick injuries in a Saudi Arabian hospital. Clin Perform Qual Health Care. 1998;6(2):79-83.
- Applebaum D, Fowler S, Fiedler N. The Impact of Environmental Factors on Nursing Stress, Job Satisfaction, and Turnover Intention. Journal of Nursing Administration. 2010;40(7/8):323-328. PMID:20661062 doi:10.1097/NNA.0b013e3181e9393b
- Guenther R, Hall A. Healthy Buildings: Impact on Nurses and Nursing Practice. Online Journal of Issues in Nursing. 2007;12(2):3-3. doi:10.3912/OJIN.Vol12No02Man02
- Jones C, Gates M. The Costs and Benefits of Nurse Turnover: A Business Case for Nurse Retention. Online Journal of Issues in Nursing. 2007;12(3):5. doi:10.3912/OJIN.Vol12No03Man04
- Delaney M. Right to Know: Reducing Risks of Fecal Pathogen Exposure for ED Patients and Staff. Journal of Emergency Nursing. 2014;40(4):352-356. PMID:24075146 doi:10.1016/j.jen.2013.07.022
- Bros A, Deboscker S, Mielcarek M. Bacteriological quality evaluation of bedpans in a university hospital. International Journal of Infection Control. 2018;14(1). doi:10.3396/IJIC.v14i1.004.18
- Qualtrics Version November, 2023. Qualtrics. 2023.
- Wonder A. Engagement in RNs Working in Magnet®-Designated Hospitals. 2012;42:575-579. PMID:23151930 doi:10.1097/NNA.0b013e318274b5a8
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing. 2022.
- Hvitfeldt E. Testdata: Download and Load Various Text Datasets. R package version 0.4.4. 2022.
- Mulvey T, Cámpoli M, Lundmark V. Establishing a Pathway to Excellence® Research Agenda: A Delphi Study to Identify Research Priorities for Evaluating Positive Practice Environments. The Journal of Nursing Administration. 2023;53(4):189-196. PMID:36916787 doi:10.1097/NNA.0000000000001269
- Mallon D, Shearwood W, Mallal S. Exposure to blood borne infections in health care workers. Med J Aust. 1992;157(9):592-5. PMID:1406418 doi:10.5694/j.1326-5377.1992.tb137397.x
 This work is licensed under a
This work is licensed under a 